Introduction
Hospital readmissions are expensive, largely preventable, and a direct measure of care quality. According to AHRQ HCUP data, Medicare patients experienced roughly 17 readmissions per 100 index admissions in 2020 - and those 2 million-plus Medicare readmissions carried an aggregate cost of $36.2 billion in that year alone.
The problem isn't that clinicians don't care about readmissions. It's that most health systems identify at-risk patients too late - after discharge, when the window for prevention has closed.
Predictive analytics changes the timing. Care teams can act before discharge - when targeted interventions still make a difference. This article covers how predictive models work in practice, what measurable improvements health systems have achieved, and what it takes to deploy these tools effectively.
Key Takeaways
- Predictive models assign individual readmission risk scores using EHR data, claims history, lab results, and social determinants of health
- Risk scores appear within clinical workflows 24–48 hours after admission, giving care teams a prioritized list of who needs intervention before discharge
- Health systems using these tools have cut preventable readmissions and reduced variable costs - with outcomes tracked at the patient level, not just the population level
- Without them, care teams rely on inconsistent, subjective case-finding - which creates wide variation in who actually receives follow-up care
- Full value requires clean data integration, population-validated models, and risk scores embedded directly in EHR workflows where clinicians already work
What Is Predictive Analytics for Hospital Readmissions?
Predictive analytics for readmissions is the use of historical and real-time patient data, processed through machine learning models, to estimate the probability that a specific patient will be re-hospitalized within 30 days of discharge.
Data sources it draws from:
- Electronic health records (diagnoses, medications, vitals, clinical notes)
- Prior hospitalization and ED utilization history
- Insurance claims and payer data
- Lab results and current clinical indicators
- Social determinants of health (SDOH) - housing stability, transportation access, social support
This is not a reporting tool. Its value lies in generating actionable risk scores that surface inside existing clinical workflows, prompting care decisions at the point of discharge or during post-discharge coordination.
Where the score lives matters as much as the score itself. Buried in a separate analytics portal that clinicians rarely open, it changes nothing. Embedded directly in the EHR discharge workflow, it changes behavior at the moment it matters.
Key Advantages of Predictive Analytics in Reducing Readmissions
The advantages below map to metrics health systems actively track: readmission rates, care costs, CMS penalty exposure, and patient outcomes. These aren't theoretical - each reflects documented operational results.
Early Identification of High-Risk Patients
Predictive models assign readmission risk scores to every inpatient based on factors including medical history, comorbidities, prior ED and inpatient utilization, demographic data, current clinical indicators, and SDOH. The output is a likelihood score for 30-day readmission.
Risk scores generated by day 2 of admission give care coordinators a prioritized list - not a gut feeling - of which patients need transition conferences, additional case management, or specialized follow-up before discharge. That changes who gets attention and when, before a preventable readmission becomes a statistic.
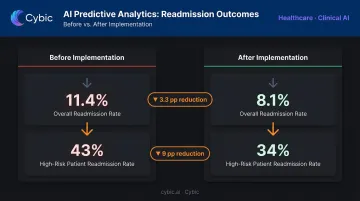
A real-world example: a regional hospital implementing an AI-based readmission prediction tool flagged the top 20th percentile of patients as high-risk, achieving sensitivity of 65% and specificity of 89%. Readmission rates dropped from 11.4% to 8.1% overall, with high-risk patient readmissions declining from 43% to 34%.
Without standardized risk stratification, clinicians rely on subjective judgment to decide who needs care coordination. One study comparing clinician assessments against LACE scores found only moderate agreement between the two (weighted kappa 0.41) - meaning physician intuition and a validated tool frequently pointed at different patients. That gap is where preventable readmissions slip through.
KPIs impacted:
- 30-day readmission rate
- Potentially preventable readmission (PPR) rate
- Care coordination utilization
- HRRP penalty exposure
- Risk stratification accuracy
Health systems with high Medicare volumes, patients managing multiple chronic conditions, or populations with limited social support see the greatest impact - these are the groups where risk concentrates and standard workflows most often miss it.
Optimized Discharge Planning and Post-Discharge Follow-Up
Effective discharge planning is one of the strongest levers for preventing readmissions. The problem is that without patient-specific risk data, discharge planning defaults to a one-size-fits-all protocol - the same generic instructions for a medically stable patient with strong social support and a complex heart failure patient living alone.
Predictive analytics makes planning specific. Examples of how risk outputs shape discharge actions:
- A patient flagged for medication non-adherence risk gets connected to a pharmacist before leaving
- A heart failure patient with a high-risk score gets a follow-up appointment within 5 days rather than 30
- High-risk patients are enrolled in telehealth check-ins or home health services before discharge, not after the first missed appointment
Allina Health, working with predictive analytics and redesigned care transitions, achieved a 27% reduction in potentially preventable readmissions for patients with clinic follow-up within 5 days of discharge, according to a Health Catalyst case study. That 5-day follow-up window is a consistent finding across multiple implementations - it's not an arbitrary threshold.
KPIs impacted:
- Post-discharge follow-up completion rate
- Days-to-first-follow-up
- Medication reconciliation rate
- 7-day and 30-day readmission rates
For patients managing two or more chronic conditions, those with prior high utilization, or patients flagged for SDOH risk factors, generic discharge processes reliably produce return visits. Risk-specific planning is what breaks that cycle.
Reduced Costs and Lower Regulatory Penalty Exposure
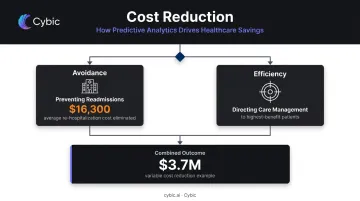
AHRQ data from 2020 puts the average readmission cost at $16,300 - 12.4% higher than the average index admission. Medicare readmissions alone totaled $36.2 billion that year.
Predictive analytics reduces costs from two directions:
- Avoidance - preventing readmissions outright eliminates the direct cost of re-hospitalization
- Efficiency - directing care management resources toward patients who will benefit most, rather than applying care management uniformly across all discharges
Allina Health reported a $3.7 million reduction in variable costs from avoided readmissions in 2015, comparing actual against expected readmissions relative to a 2013 baseline (via Health Catalyst case study data). A separate Allina reporting line attributed $3.2 million in variable cost savings to avoiding 420 readmissions through enhanced care transitions.
Beyond direct cost, hospitals with excess readmission rates face CMS Hospital Readmissions Reduction Program (HRRP) penalties - payment reductions capped at 3% of Medicare inpatient payments. For large health systems, 3% of Medicare revenue is not a rounding error. Reducing readmissions improves both the penalty calculation and the broader value-based care scorecard simultaneously.
KPIs impacted:
- Cost per episode of care
- Avoided readmission variable costs
- HRRP penalty amount
- Care management cost efficiency
- Value-based contract performance scores
The financial advantage compounds at scale. Health systems managing thousands of annual discharges and those heavily dependent on Medicare reimbursement see the greatest ROI from systematic deployment.
What Happens Without Predictive Analytics in Readmission Management
Operating without predictive tools means relying on inconsistent, subjective case-finding. That gap produces a predictable pattern of compounding problems:
- High-risk patients get discharged without targeted follow-up, and some return through the ED within days - consuming bed capacity and care resources that could have gone elsewhere.
- Care teams spend time managing returning patients rather than preventing returns, compounding workload without improving outcomes.
- HRRP penalty risk stays unresolved because no systematic mechanism exists to identify the patients driving excess readmissions - and financial exposure from repeated hospitalizations keeps building.
- Value-based care performance erodes when organizations can't identify which interventions are working or which patient populations need a different approach.
The before/after data from real implementations illustrates the gap directly. Before an AI readmission tool was implemented at one regional hospital, overall readmission rates sat at 11.4% and high-risk patient readmissions at 43%. After implementation, those figures dropped to 8.1% and 34%, respectively. Those percentage-point reductions represent patients who didn't return within 30 days. Each avoided readmission eliminates a cost exceeding $16,000 per episode.
How to Get the Most Value from Predictive Analytics
Predictive analytics delivers its full value only when embedded into clinical workflows. A risk score that clinicians have to retrieve from a separate platform - one they need to log into outside their normal EHR workflow - will rarely be used consistently enough to change outcomes.
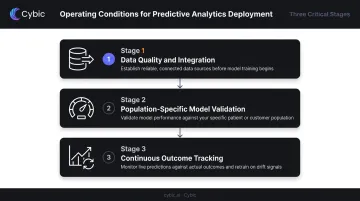
Three operating conditions determine whether implementations succeed or stall:
1. Data quality and integration Models are only as reliable as the data feeding them. Health systems need a centralized data architecture that pulls from EHRs, claims data, and SDOH sources consistently and without gaps.
Platforms like Cybic's Drava address this directly - unifying data ingestion, machine learning, AI reasoning, and intelligent agents into a single governed architecture. Critically, Drava is designed to integrate with existing infrastructure rather than requiring health systems to rebuild it.
2. Population-specific model validation A model validated on one patient population can underperform when applied to another. Validated tools like the HOSPITAL score and LACE index offer strong starting baselines: the HOSPITAL score achieved a C-statistic of 0.72 across more than 117,000 patients in international validation.
Even so, custom models built on a health system's own data - and reviewed as demographics shift - will consistently outperform generic tools.
3. Continuous outcome tracking Readmission rates, care coordination completion rates, and cost savings should be monitored against model predictions continuously. If a model's performance drifts - which happens as patient populations change - that signal needs to surface before it translates into missed interventions. MLOps practices, including automated model monitoring and retraining pipelines, make this sustainable at scale.
Conclusion
Predictive analytics for readmissions is a practical operational tool - not a technology experiment. It gives care teams the ability to act on data before patients leave the hospital rather than reacting when they return.
Each discharge becomes an opportunity to direct the right resources to the right patients: targeted follow-up for those who need it, streamlined transitions for those who don't. Across thousands of annual discharges, that precision compounds - measurably lower readmission rates, reduced CMS penalty exposure, and care management capacity concentrated where it produces outcomes.
Health systems that treat readmission risk as a data problem - not just a care coordination challenge - consistently outperform those that don't. The difference shows up in benchmarks, in penalty calculations, and in how efficiently clinical resources get deployed.
Frequently Asked Questions
What data does predictive analytics use to assess hospital readmission risk?
Predictive models draw from EHRs, prior hospitalization records, lab results, medication history, insurance claims, and social determinants of health such as housing stability and transportation access. The breadth and quality of this data directly determines how accurately the model predicts individual patient risk.
How accurate are predictive models in identifying high-risk patients?
Validated tools like the HOSPITAL score show C-statistics of 0.72–0.75 in large multi-center studies; custom EHR-integrated models have reached AUCs of 0.78–0.81 in real implementations. Accuracy varies by design and patient population, so all models should be validated locally before deployment.
What is the HRRP and how does it penalize hospitals for readmissions?
The Hospital Readmissions Reduction Program is a CMS initiative that reduces Medicare payments to hospitals with excess readmission rates for specified conditions including heart failure, COPD, pneumonia, and AMI. Payment reductions are capped at 3%, creating a direct financial incentive for health systems to manage readmission performance.
How do hospitals integrate predictive analytics into existing EHR systems?
Integration embeds risk scores directly into EHR dashboards, surfacing readmission risk during routine documentation rather than in a separate platform. This requires a data pipeline connecting multiple source systems to a validated model with outputs available at the point of care.
What are the biggest barriers to implementing predictive analytics for readmission prevention?
The three most common barriers are inconsistent or incomplete data across source systems, clinician trust and adoption of model outputs, and the technical challenge of embedding predictions into clinical workflows without disrupting existing processes.
Can predictive analytics eliminate all hospital readmissions?
No - some readmissions are clinically necessary and appropriate. Predictive analytics targets avoidable readmissions by enabling earlier, more targeted interventions for patients at elevated risk for preventable returns. The goal is reducing that subset, not eliminating readmissions entirely.