Introduction: Why Healthcare Data Analytics Is No Longer Optional
Healthcare organizations are generating data at a scale that would have seemed implausible a decade ago. EHRs, billing systems, wearables, medical devices, patient engagement platforms - the sources keep multiplying. Yet most of it goes unanalyzed. According to the World Economic Forum, 97% of hospital data produced each year goes unused. The volume was never the problem.
The problem is fragmentation. Data sits in siloed systems that were never designed to talk to each other. Governance is inconsistent.
Reports are static, backward-looking, and disconnected from the decisions clinicians and operators need to make right now. The cost shows up in preventable readmissions, uncollected revenue, overstretched staff, and missed care opportunities.
This guide covers what healthcare data analytics actually is, where it delivers the highest value, how to build a strategy that works, and what to look for in a partner who can turn data into operational action.
Key Takeaways
- 97% of hospital data goes unused - the problem is fragmentation, not volume
- Highest-impact use cases: readmission prediction, sepsis alerts, denial prevention, and workforce forecasting
- Strategy must start with business objectives, not technology selection
- Governance and compliance belong at the architecture level - not retrofitted post-deployment
- Insights only drive outcomes when they surface inside the workflows clinicians and operators already use
What Is Healthcare Data Analytics?
Healthcare data analytics covers the collection, integration, and analysis of clinical, operational, and financial data to generate insights that improve patient outcomes, reduce costs, and optimize operations.
That's a broader mandate than reporting or dashboarding - which only describe what already happened. Analytics explains why it happened, predicts what will happen next, and at the highest maturity level, recommends what to do about it.
The Data Landscape
Healthcare organizations manage data from a wide range of systems that rarely communicate cleanly:
- EHRs - clinical notes, lab results, diagnoses, medication records
- Billing and claims systems - charges, payer adjudication, denial data
- Scheduling and staffing platforms - shift data, patient volume, acuity metrics
- Medical devices and monitoring systems - real-time vitals and alerts
- Patient engagement tools - appointment data, satisfaction scores, outreach history
- Imaging and genomic data - high-volume, often unstructured
ONC data shows that while 96% of non-federal acute care hospitals have adopted certified EHRs, only 70% of hospitals engaged in all four domains of interoperable exchange in 2023. Digitization is largely complete. Getting those systems to share data reliably is a different challenge entirely.
The Four Levels of Analytics Maturity
| Level | Question Answered | Example |
|---|---|---|
| Descriptive | What happened? | Readmission rate last quarter |
| Diagnostic | Why did it happen? | Drivers of readmissions by condition |
| Predictive | What will happen? | Which patients are at risk before discharge |
| Prescriptive | What should we do? | Automated care intervention trigger |
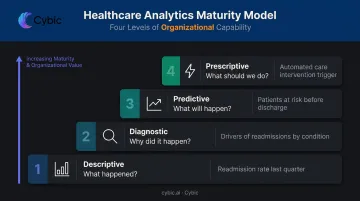
Most healthcare organizations are still operating at the descriptive level - producing reports that confirm what happened after the fact, with limited ability to act on patterns before they become problems.
Grand View Research estimates the US healthcare analytics market at $21.21 billion in 2024, projected to reach $67.48 billion by 2033. Investment is accelerating because organizations that move up the maturity curve gain a measurable competitive and financial advantage.
Key Use Cases: Where Healthcare Data Analytics Delivers the Most Value
Analytics creates value only when it connects to real workflows - not when it lives in a reporting layer that clinicians and operators rarely open. The highest-ROI use cases share one characteristic: the insight triggers an action inside an existing system.
Clinical and Patient Outcomes
Readmission prediction is one of the most financially grounded use cases in clinical analytics. The average readmission costs $16,300 - more than the $14,500 average for an initial admission - and CMS's Hospital Readmissions Reduction Program (HRRP) can reduce Medicare payments by up to 3% for hospitals with excess readmissions.
Predictive models trained on EHR data, lab results, and social determinants of health can identify high-risk patients before discharge and trigger proactive interventions. One peer-reviewed implementation study found an AI-based readmission clinical decision support tool was associated with a 25% relative reduction in readmissions, dropping the rate from 11.4% to 8.1%.
Clinical decision support (CDS) takes this further by embedding analytics directly into EHR workflows. Sepsis alerts, medication safety flags, and evidence-based care pathway recommendations surface where clinicians are already working - no separate dashboard required.
The stakes are concrete: at least 1.7 million US adults develop sepsis annually, and at least 350,000 die or are discharged to hospice. A sepsis early warning system (TREWS) showed unadjusted mortality of 14.6% for patients whose alerts were confirmed and acted on, versus 19.2% for those whose alerts were not - a gap that only closes when the model is wired into the care workflow.
Operational and Financial Performance
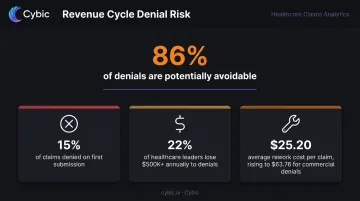
Revenue cycle management (RCM) analytics targets one of the most preventable sources of financial loss in healthcare. Private payers deny nearly 15% of claims on first submission, and 60% of medical group leaders reported higher denial rates in 2024 than the prior year. Perhaps most striking: 86% of denials are potentially avoidable, according to a Change Healthcare analysis.
The financial exposure is real:
- 22% of healthcare leaders lose at least $500,000 annually to denials
- 1 in 10 lose more than $2 million
- Average administrative rework costs $25.20 per claim, rising to $63.76 for commercial denials
Predictive models that score claims for denial risk before submission - combined with automated coding scrubbing and payer contract analysis - address this upstream rather than chasing denials after they land.
Workforce forecasting addresses the labor cost side of the same equation. When Memorial Hermann built an internal staffing agency supported by analytics-driven forecasting, they cut travel agency spend by 50% in 2022 while improving nurse experience. Integrating scheduling data, historical patient volume, and acuity metrics allows health systems to match staffing to actual demand at the shift and unit level - reducing premium labor costs without burning out permanent staff.
Population Health and Preventive Care
Chronic and mental health conditions account for 90% of the nation's $4.9 trillion in annual healthcare expenditures, according to the CDC. Population health analytics addresses this by identifying cohorts at risk before they need acute care. In practice, that means:
- Stratifying chronic disease risk across patient populations
- Forecasting disease prevalence by demographic and geography
- Enabling proactive care management before conditions escalate
The ACO model illustrates the financial case for prevention. CMS reported the Medicare Shared Savings Program generated more than $2.1 billion in net savings in 2023, the largest in program history. Analytics-driven care gap closure and risk stratification are what make proactive management programs feasible to run across thousands of patients.
Building a Healthcare Data Analytics Strategy: A Step-by-Step Framework
Most healthcare analytics initiatives fail not because of bad technology, but because they start with technology selection rather than problem definition. The right sequence matters.
Step 1: Define Measurable Business Objectives
Strategy must begin with scoped, outcome-oriented goals - not vague directives like "implement analytics." Examples of well-defined objectives:
- Reduce 30-day readmissions by 15% within 12 months
- Cut claim denial rates from 8% to under 4%
- Reduce travel nurse spend by 30% through improved shift forecasting
Each objective needs a named executive sponsor and clearly defined KPIs. Without that anchor, analytics programs drift toward generating reports nobody acts on.
Step 2: Conduct a Data and Infrastructure Assessment
Before selecting any platform or tool, map what you have:
- Data sources - which systems exist and what data they produce
- Siloes and quality gaps - duplicates, missing fields, inconsistent coding standards
- Integration capabilities - existing FHIR APIs, HL7 interfaces, data warehouse infrastructure
- Interoperability gaps - where data flow breaks between systems
This assessment determines what's buildable in the near term versus what requires infrastructure work before analytics can be layered on top.
Step 3: Prioritize Governance and Compliance Architecture
Governance cannot be retrofitted after deployment. It must be embedded at the architecture level from day one. A healthcare data governance framework should cover:
- HIPAA-compliant data handling - privacy rule compliance for PHI
- Role-based access controls (RBAC) - restricting data access by role, not just by system
- Audit trails - complete logs of who accessed what and when
- Master data management - standardized patient, provider, and facility identifiers across systems
- Data stewardship roles - named accountability for data quality across departments
- Data lineage tracking - understanding where data originates and how it transforms

This is also the foundation for responsible AI deployment. Organizations that skip this step find themselves unable to validate AI outputs or explain why a risk alert fired - creating both clinical and regulatory exposure.
Step 4: Start with a Focused Pilot, Then Scale
Enterprise-wide deployment from day one is a reliable path to failure. A single, high-impact, measurable use case - sepsis alerting, denial prediction, readmission risk scoring - delivers faster results and surfaces integration issues before they become enterprise-scale problems.
A successful pilot accomplishes three things:
- Proves ROI in concrete, measurable terms
- Builds organizational confidence and clinical buy-in
- Creates a replicable architecture for subsequent use cases
Step 5: Integrate Insights Into Operational Workflows
This is where most organizations plateau. The gap between analytics investment and realized value is widest here - and it's almost entirely an integration problem, not a modeling one.
Analytics must trigger actions within existing systems:
- Risk scores surfacing inside EHR workflows, not separate portals
- Staffing signals feeding directly into scheduling tools
- Denial risk flags populating RCM queues before claim submission
Engineering this integration is harder than building the underlying models. It requires deep knowledge of how clinical and operational systems are structured, what APIs they expose, and how to embed outputs without disrupting existing workflows.
Cybic's healthcare analytics engagements are structured around this exact challenge: connecting data pipelines, ML outputs, and AI reasoning directly into EHR, RCM, and scheduling systems - so insights reach the people who act on them, at the moment they need to.
Data Governance, Compliance, and Security in Healthcare Analytics
The Regulatory Framework
Healthcare analytics operates within a strict compliance environment:
- HIPAA Privacy and Security Rules - governing PHI access, use, and disclosure
- HITECH Act - extending HIPAA requirements to business associates and strengthening enforcement
- ONC HTI-1 Final Rule - establishing transparency requirements for AI and predictive algorithms in certified health IT
- NIST AI RMF - defining trustworthy AI characteristics including validity, reliability, accountability, explainability, and fairness
Non-compliance carries real consequences. HHS OCR resolved compliance reviews in 2024 totaling over $8.7 million in settlements and penalties. Separate from enforcement costs, IBM's 2023 Cost of a Data Breach Report puts the global average breach cost at $4.45 million - a figure that doesn't include reputational damage or care disruption.
What Good Governance Looks Like in Practice
The components of a functional healthcare data governance framework:
- Standardized metric definitions - so "30-day readmission rate" means the same thing across systems and reports
- Data quality monitoring - continuous checks for missing fields, duplicates, and coding inconsistencies
- Lineage tracking - knowing exactly where every data point originates
- Encryption in transit and at rest - for all PHI
- RBAC and audit trails - enforced at the platform level, not by policy alone
These aren't administrative overhead. They're what make analytics outputs trustworthy enough to act on clinically and financially.
Governing AI Specifically
Traditional data governance handles structured data well. AI adds a layer of risk that standard frameworks weren't designed for:
- Model drift - predictive models degrade over time as patient populations and care patterns shift
- Bias monitoring - models trained on historical data can encode historical disparities
- Explainability - clinicians need to understand why a risk alert was triggered, not just that it was
ONC's HTI-1 requirements and the NIST AI RMF both require governance embedded by design - meaning bias checks, audit trails, and explainability built into the architecture before deployment, not retrofitted after. When evaluating analytics platforms or partners, the practical question is whether those controls exist at the system level or only in policy documentation.
What to Look for in a Healthcare Data Analytics Partner
The right partner doesn't just understand data - they understand healthcare data specifically and can build systems that operate inside your existing infrastructure.
Key evaluation criteria:
- Healthcare domain expertise - proven experience with EHR integration, HIPAA compliance architecture, and clinical workflow design, not just general data engineering
- Engineering-led delivery - a focus on building and deploying working systems rather than issuing recommendations and handing off implementation to your team
- Works across cloud, hybrid, or on-prem environments without locking you into a single vendor ecosystem
- Governance embedded by design - RBAC, encryption, audit trails, and model explainability incorporated at the architecture level, not applied as a compliance layer afterward
- Connects to EHRs, RCM platforms, and scheduling tools from day one, rather than delivering standalone dashboards
The last point is where many engagements fall short. A partner who delivers an accurate predictive model that requires staff to navigate a separate interface will generate limited adoption and limited ROI. The goal is analytics that surfaces inside the systems where clinical and operational decisions already happen.
That adoption gap is what shapes how Cybic structures its engagements. Rather than delivering models or dashboards in isolation, Cybic connects data pipelines, ML models, and AI reasoning agents into unified operational systems. Governance and security controls - RBAC, encryption, audit trails - are embedded at the architecture level from the start, across cloud, hybrid, and on-prem environments.
Frequently Asked Questions
What is healthcare data analytics and how is it different from traditional healthcare reporting?
Traditional reporting describes what already happened - a static snapshot of historical performance. Healthcare data analytics integrates clinical, operational, and financial data to generate predictive and prescriptive insights that drive real-time and strategic decisions. The distinction: analytics drives decisions; reporting only records them.
What are the most impactful use cases of data analytics in healthcare?
The highest-ROI use cases are patient risk stratification, clinical decision support (especially sepsis detection), revenue cycle denial prevention, workforce forecasting, and population health management. Impact depends on embedding insights directly into clinical and operational workflows - not in separate dashboards.
How do healthcare organizations ensure HIPAA compliance in their analytics programs?
Compliance requires role-based access controls, encryption in transit and at rest, audit trails, data lineage tracking, and a defined data stewardship framework. The most important factor is selecting platforms and partners that embed these controls at the architecture level rather than applying them as a post-deployment layer.
What is the difference between predictive and prescriptive analytics in healthcare?
Predictive analytics forecasts what is likely to happen - such as identifying patients at high readmission risk before discharge. Prescriptive analytics recommends or automates the optimal response: adjusting staffing based on real-time acuity, or triggering care management outreach automatically. Most organizations are still maturing toward prescriptive capability.
How long does it take to implement a healthcare data analytics strategy?
A focused pilot targeting a single use case can deliver measurable results within 60–90 days. Enterprise-wide implementation spans 12–24 months, with governance and data quality work front-loaded before broader deployment.
What should healthcare organizations look for in a data analytics consulting partner?
Prioritize engineering-led delivery over advisory-only engagements, governance embedded by design, proven experience integrating with healthcare systems, and the ability to build systems that surface insights inside existing clinical and financial workflows - not alongside them.