Introduction
Healthcare organizations generate enormous volumes of patient, operational, and clinical data. Yet the quality and governance of that data routinely fall short of what safe, compliant care delivery requires.
A recent Deloitte survey of 100 US healthcare technology executives found that only 32% reported reduced friction from data quality concerns. The majority still work with data they can't fully trust.
The consequences aren't abstract. Poor data governance produces clinical errors, HIPAA violations, denied claims, and analytics that leaders actively distrust. A single patient appearing under three different name formats across registration, radiology, and pharmacy isn't a minor IT issue - it's a patient safety risk.
This guide gives healthcare leaders a practical framework for governing patient and operational data effectively. It covers the core pillars, compliance obligations, a step-by-step implementation approach, and why AI systems now require the same governance rigor as the data they consume.
Key Takeaways
- Healthcare data governance defines the policies, roles, and processes that keep patient data accurate, secure, accessible, and compliant.
- Weak governance causes clinical errors, HIPAA violations, denied claims, and eroded confidence in data-driven decisions.
- Effective frameworks rest on five pillars: data quality, access control, regulatory compliance, stewardship, and standardization.
- Start narrow - one data domain or department - then scale using early wins to build momentum and secure continued funding.
- AI in clinical and operational workflows needs governance controls embedded in the architecture from day one.
What Is a Healthcare Data Governance Framework (and Why It Matters)
Healthcare data governance is the structured set of policies, procedures, roles, and standards that govern how patient and operational data is collected, accessed, used, and protected across its full lifecycle.
That definition sounds similar to general data management - but healthcare introduces a tension that most industries don't face at the same scale: the need to enforce strict privacy protections while simultaneously ensuring clinical staff can access information fast enough to make care decisions.
Why Healthcare Is Uniquely Hard
Data in a typical health system originates from dozens of siloed sources, each with its own identifiers and terminology:
- Electronic health records (EHRs)
- Laboratory and imaging systems
- Billing and revenue cycle platforms
- Pharmacy management systems
- Patient portals and remote monitoring devices
These systems often don't agree on basic facts. A single patient might appear as "Robert Johnson" in registration, "R. Johnson" in radiology, and "Bob Johnson" in pharmacy. Without governance, those three records may never be linked. A clinician making a medication decision is then working with an incomplete picture of that patient's history.
Governance vs. Data Management
These two terms are often used interchangeably, but the distinction matters:
- Data governance defines the rules: the policies, roles, and standards that determine how data should be handled and by whom.
- Data management covers the execution: the systems and technical practices that carry those policies out in daily operations.
Both are necessary. Governance without management produces policies no one can actually implement. Management without governance means teams build capable systems with no shared rules - leading to inconsistent data handling and gaps in accountability that surface at the worst possible moments.
The Key Pillars of a Healthcare Data Governance Framework
Healthcare organizations differ in size, structure, and maturity - but high-functioning governance programs share the same core pillars.
Data Quality and Integrity
Data quality governance starts with defining what "good data" looks like at the organizational level - accuracy, completeness, timeliness, and consistency - and then building formal processes to detect errors, flag duplicates, and correct records before they reach clinical workflows.
The stakes are real. A 2020 JAMA Network Open study of nearly 23,000 patients across three major health systems found that 21.1% of patients who read their own ambulatory visit notes reported a mistake. Of those, 42.3% considered the error serious and 9.9% considered it very serious.
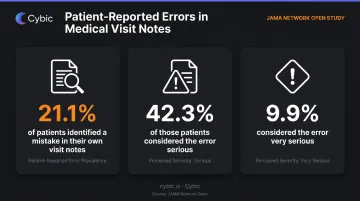
Patients are catching mistakes that clinicians missed - a governance failure, not just a documentation problem.
Data Security and Access Control
Role-based access control (RBAC) is the foundation here: defining who can view, modify, or export patient data based on their job function - not blanket permissions applied to entire departments.
HIPAA's "minimum necessary" standard sets the expectation: staff access only what their specific role requires. The practical challenge is clinical reality - emergency scenarios where a provider needs access beyond normal permissions, and where rigid controls create dangerous friction.
Well-designed governance anticipates these exceptions with defined override procedures that are logged and reviewable, rather than simply granting broad access to avoid the problem.
Regulatory Compliance and Auditability
Governance must generate auditable evidence - access logs, change histories, and documented workflows - that can demonstrate compliance to regulators on demand. Without this, organizations cannot prove who accessed which data, when, and for what purpose.
That traceability is a core HIPAA requirement. It also matters increasingly under state-level privacy laws, which continue to expand and tighten regardless of federal regulatory changes.
Data Stewardship and Accountability
A data steward owns a specific data domain - patient demographics, clinical documentation, financial records - with actual authority to enforce quality standards and resolve disputes about data definitions.
The word "authority" matters. Organizations consistently create stewardship roles with responsibility but no decision rights, then wonder why definitions go unenforced. Governance without accountable owners fails - without exception.
Data Standardization and Business Glossaries
Terminology conflicts across departments corrupt analytics in ways that are hard to detect. "Admission date" means something different to registration, clinical staff, and billing. When those definitions diverge unnoticed, cross-department reports produce numbers that don't reconcile - and nobody can agree on which number is correct.
A formal business glossary standardizes:
- Term definitions and their authoritative sources
- Which system owns each data element
- Update frequencies and data quality thresholds
- Metadata that allows analysts to trace a business term to its source system
The glossary must be accessible to all staff and integrated into the data catalog - not buried in a SharePoint folder that nobody opens.
HIPAA Compliance and Regulatory Requirements in Healthcare Data Governance
The HIPAA Security Rule organizes protections for electronic protected health information (ePHI) into three categories of safeguards:
| Safeguard Type | What It Covers |
|---|---|
| Administrative | Policies, workforce training, risk analysis and management |
| Physical | Facility access controls, workstation security, device controls |
| Technical | Encryption, audit logs, automatic logoff, access controls |
HIPAA doesn't mandate specific technologies. It requires organizations to demonstrate that appropriate controls are in place and actively managed - a distinction that regularly surfaces as a compliance gap during audits.
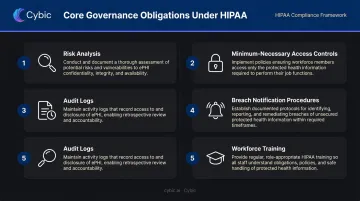
Core Governance Obligations Under HIPAA
- Conduct and document formal risk analyses
- Implement minimum-necessary access controls with defined role permissions
- Maintain audit logs identifying who accessed ePHI and when
- Establish breach notification procedures with documented timelines
- Train all workforce members who handle patient information, and document that training
What Non-Compliance Actually Costs
The enforcement record is instructive. The OCR settled with Memorial Healthcare System for $5.5 million after failures in audit controls allowed unauthorized access to patient records - a case OCR explicitly described as highlighting the importance of access monitoring. Presence Health paid $475,000 in the first HIPAA enforcement action specifically for untimely breach notification.
These cases aren't outliers. Each one traces back to a specific governance failure: missing audit controls, undefined response processes, or delayed notification. The same gaps appear across organizations of every size.
Those gaps become even more consequential for organizations operating across borders.
HIPAA vs. GDPR: Two Separate Obligations
Organizations working with international data or serving EU populations face both frameworks simultaneously, but with different requirements:
- HIPAA: Breach notification must occur without unreasonable delay and no later than 60 days after discovery.
- GDPR Article 33: Notification to the supervisory authority is generally required within 72 hours of becoming aware of the breach.
These are separate obligations with separate timelines. Healthcare technology vendors serving EU populations cannot treat HIPAA compliance as a substitute for GDPR compliance.
How to Build Your Healthcare Data Governance Framework: A Step-by-Step Approach
Governance programs most commonly fail because they start too broad. Gartner predicted in 2024 that 80% of data and analytics governance initiatives will fail by 2027 due to lack of a real or manufactured crisis - a general benchmark, but one that matches the pattern AHIMA documents in healthcare information governance programs specifically.
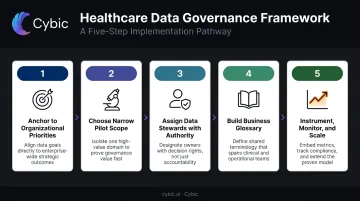
Step 1: Anchor Governance to Organizational Priorities
Governance done for its own sake rarely survives the planning phase. The program needs an explicit connection to something the executive team already cares about: reducing adverse drug events, improving referral accuracy, cutting denied claims, or meeting a population health target.
Without that anchor, governance competes against clinical and operational priorities - and loses.
Step 2: Choose a Visible, Narrow Pilot Scope
Pick a single data domain - patient identity/MPI or medication reconciliation work well - in one department or facility. Narrow scope creates the conditions for working processes to be established before scaling.
The goal is a quantified win: duplicate records reduced, hours saved on manual reconciliation, audit findings resolved. Conceptual progress doesn't secure the next budget cycle. Numbers do.
Step 3: Assign Data Stewards with Real Authority
The most common governance failure mode: assigning responsibility without authority. Stewards need organizational standing to enforce definitions, reject non-compliant data entries, and escalate disputes.
Roles best suited for stewardship in healthcare include:
- Clinical informatics leads
- Health Information Management (HIM) directors
- Revenue cycle managers
- Quality and compliance officers
Document stewardship responsibilities and decision rights in a formal governance charter - AHIMA's practice brief guidance outlines what that charter should cover.
Step 4: Build a Business Glossary and Standardize Definitions
Convene cross-functional working sessions with clinical staff, IT, compliance, and revenue cycle to resolve definitional conflicts. This takes longer than anyone expects - most organizations discover that five departments use the same term to mean five different things.
The glossary that emerges becomes the single authoritative source. To be effective, it needs to:
- Be searchable and accessible to all staff
- Link directly to the data catalog
- Allow users to trace any business term back to its source system
Step 5: Instrument, Monitor, and Scale
Once the pilot delivers measurable results, governance shifts from a project into an ongoing operational function. This means:
- Establishing regular audit cycles with defined owners
- Assigning ongoing data quality monitoring responsibilities
- Using early participants as mentors who carry governance practices into new departments
- Treating every system implementation, acquisition, or regulatory change as a trigger to review and update governance processes
AHIMA frames information governance as a multi-year initiative that evolves from scoped projects into a sustained program. The measure of success is increasing maturity over time, not a single point of completion.
Common Pitfalls That Derail Healthcare Data Governance Programs
Three failure patterns appear consistently across healthcare organizations:
- Scope creep before value delivery : the program expands during planning until it becomes too large to execute, and no quick wins materialize to justify continued investment.
- Nominal executive sponsorship : leaders endorse governance in principle but don't visibly champion it when it competes for budget or staff time. AHIMA identifies executive sponsorship as a critical success factor specifically because sponsors must provide funding and oversight, not just a name on the charter.
- Stewards without authority - definitions get established on paper but ignored in practice because stewards have advisory roles, not decision rights.
The Cultural Problem That Tools Cannot Solve
No governance platform resolves the deeper issue: clinical staff, IT teams, and administrators must share a working understanding of why data standards affect patient outcomes and organizational performance. Organizations that treat governance as an IT project underdeliver. Cultural alignment has to come from operations, not the technology team.
That gap is exactly where tool-first approaches go wrong. Purchasing governance software without a governance strategy is a common mistake. Tools provide scalability and auditability - but they cannot define who owns a data domain, settle a dispute about what "active patient" means, or make a CMIO care about data quality. Those outcomes depend on governance committee cadence, clear escalation paths, and budget protection that leadership actively defends.
The Role of AI Governance in a Modern Healthcare Data Framework
As healthcare organizations deploy AI and machine learning for clinical decision support, predictive risk scoring, and operational automation, those models need governance with the same rigor applied to the data they consume.
The ONC's HTI-1 rule makes this explicit: predictive decision support interventions require 31 documented source attributes, plus risk analysis, risk mitigation, governance processes, bias management, and ongoing local validity and fairness monitoring.
What Happens Without Governance
A 2019 study by Obermeyer et al. found that a widely used population-health algorithm exhibited significant racial bias because it used health costs as a proxy for health needs - a proxy that encoded unequal access to care. Correcting the bias would have increased the percentage of Black patients receiving additional care from 17.7% to 46.5%. The algorithm was affecting millions of patients before the disparity was identified.
An ungoverned AI model can replicate systemic disparities at scale. Without audit trails and bias monitoring, organizations cannot detect the problem - let alone demonstrate to regulators or patients how a clinical recommendation was generated.
Governance Embedded by Design
For healthcare organizations deploying AI, "governance by design" means controls are architectural, not cosmetic. In practice, this includes:
- Restrict model invocation with RBAC - defining which users and systems can call AI models
- Encrypt data at rest and in transit across all pipeline layers
- Log AI-driven recommendations alongside the inputs that generated them, creating a complete audit trail
- Prevent proprietary clinical data from training external models without explicit authorization
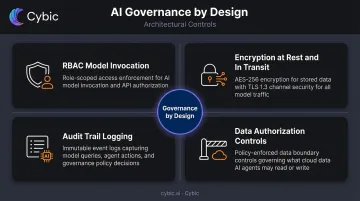
Cybic's Drava platform is built around this approach. As an enterprise data intelligence to automation platform, Drava connects data pipelines, ML models, AI reasoning, and intelligent agents within a governed architecture: RBAC, encrypted data protection, auditability of AI-driven actions, and HIPAA compliance are built into the foundation, not bolted on after deployment.
For healthcare organizations balancing AI capability with regulatory accountability, that difference matters. Retrofitted compliance creates gaps that audits - and regulators - will find.
Frequently Asked Questions
What are the key pillars of a healthcare data governance framework?
The five core pillars are data quality and integrity, security and access control, regulatory compliance and auditability, data stewardship and accountability, and data standardization. Mature organizations typically add a sixth pillar covering AI and analytics governance as models become embedded in clinical and operational workflows.
How does HIPAA compliance relate to data governance in healthcare?
HIPAA establishes the minimum legal requirements for protecting ePHI. Data governance is the operational framework through which organizations consistently meet those requirements - not just during audits, but daily through documented policies, role-based access controls, audit logging, and workforce training.
What is the difference between data governance and data management in healthcare?
Governance is the strategy: the rules, roles, and policies that define how data should be handled. Data management is the execution: the systems and processes that put those rules into action. Both are required. Without management, governance policies go unenforced. Without governance, management systems operate without consistent rules.
How do you get executive buy-in for a healthcare data governance program?
Connect governance objectives to a priority leadership already owns - reducing denied claims, improving patient safety metrics, or meeting a specific regulatory deadline. Framing governance as a means to a strategic end, rather than an IT initiative, is more effective than leading with compliance or data quality arguments alone.
What role does AI governance play in a healthcare data governance framework?
AI systems processing clinical data must be governed like the data itself - with documented model inputs and outputs, access controls, bias monitoring, and audit trails. Without these controls, organizations cannot explain AI-driven decisions to regulators or patients, and cannot detect when a model begins producing biased or degraded outputs.
How long does it take to implement a healthcare data governance framework?
A scoped pilot focused on one data domain can produce measurable results within a few months, but enterprise-wide governance is a multi-year journey. AHIMA frames information governance as an evolving program - one that must adapt continuously as systems change, regulations update, and new data sources are added.