Introduction
Clinical teams across the US are spending more time on documentation than on patients. A 2023 JAMA Network Open study found that primary care physicians spend a median 36.2 EHR minutes per visit - including after-hours "pajama time" - while direct clinical face time gets a fraction of the workday. That imbalance has real consequences: delayed care, rising denial rates, and clinician burnout that accelerates turnover.
Those consequences are showing up in metrics healthcare organizations already track. AI-powered clinical document analysis is actively moving those numbers - documentation time, clean claim rates, audit response time, and physician satisfaction scores.
This article covers what AI clinical document analysis actually does, where it delivers measurable results, what organizations lose by operating without it, and how to implement it effectively.
Key Takeaways
- AI clinical document analysis uses NLP, machine learning, and large language models to automatically extract, structure, and route information from clinical documents
- Its clearest operational benefits are reduced documentation time, improved coding accuracy, faster revenue cycle performance, and stronger compliance readiness
- Without it, organizations face rising denial rates, audit exposure, inconsistent documentation quality, and documentation-driven burnout with no release valve
- Consistent application compounds the value: governance, provider oversight, and outcome tracking are what separate durable gains from one-time wins
- The purpose is straightforward - free providers from administrative friction so clinical judgment can do its actual job
What Is AI-Powered Clinical Document Analysis?
AI-powered clinical document analysis uses artificial intelligence - specifically NLP, machine learning, and large language models - to automatically read, interpret, and extract data from clinical documents. The output is structured, actionable information from records that would otherwise require manual review.
Where It Applies Across the Care Continuum
The technology touches nearly every documentation-heavy workflow in healthcare:
- Ambient charting - AI listens to patient-provider conversations and generates structured clinical notes in real time
- Medical coding support - NLP models match diagnoses and procedures to ICD-10 and CPT codes from unstructured notes
- Prior authorization drafting - AI pre-populates PA requests from existing patient data, reducing manual assembly time
- Discharge summary generation - Automated drafting tools compile relevant clinical details into structured summaries
- Referral triage - AI extracts and routes key clinical information from referral letters to the appropriate care team
- Audit documentation - Structured outputs create traceable, consistently formatted records ready for payer or regulatory review

Accurate clinical information available faster, with less manual effort, means care teams can act on it sooner and spend less time reconstructing it later.
Key Advantages of AI-Powered Clinical Document Analysis
These advantages reflect operational outcomes that healthcare leaders and clinical teams actually measure. Gains build with consistent application and structured governance - not just at go-live.
Advantage 1: Reduced Documentation Burden and Provider Time Recovery
The baseline problem is well-documented. Physicians spend a median 36.2 EHR minutes per visit, and according to the AMA's 2025 prior authorization survey, physicians complete roughly 40 prior authorizations per week, consuming 13 hours of practice time weekly - with 95% reporting care delays as a direct result.
AI clinical document analysis addresses this on multiple fronts:
- Ambient documentation tools generate structured clinical notes from recorded conversations, reducing post-visit charting time
- NLP models extract diagnoses, medications, and clinical findings from existing records without manual entry
- Automated drafting tools pre-populate prior authorization forms and referral letters from existing patient data
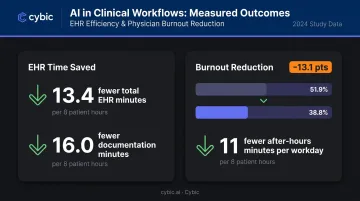
The time recovery is real and measurable. A multisite JAMA study of 8,581 ambulatory clinicians found AI scribe adoption associated with 13.4 fewer total EHR minutes and 16.0 fewer documentation minutes per 8 scheduled patient hours. A separate 30-day study found burnout fell from 51.9% to 38.8% after ambient AI scribe adoption, with after-hours documentation dropping by nearly 11 minutes per workday.
KPIs impacted: Hours on documentation per provider per day, after-hours EHR time, burnout scores, patient encounters per session
When it matters most: High-volume primary care, rural or understaffed systems where documentation overhead falls on fewer providers, organizations where EHR complexity creates charting friction at scale
Advantage 2: Higher Documentation Accuracy and Coding Performance
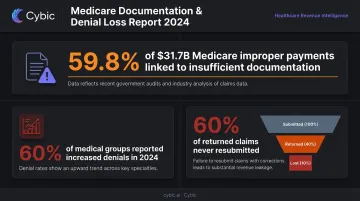
Incomplete documentation is a financial problem, not just an operational one. CMS reported $31.70 billion in Medicare FFS improper payments in FY2024 - and 59.8% of those improper payments were tied to insufficient documentation, with another 10.0% attributed to incorrect coding. That's roughly 70% of Medicare improper payment exposure tied directly to documentation quality.
AI document analysis closes this gap by:
- Reading clinical notes and suggesting appropriate ICD-10 and CPT codes based on documented findings
- Flagging incomplete or inconsistent documentation before a claim is submitted
- Extracting structured data from unstructured notes so coding reflects the full clinical picture, not just the most recently entered details
AI systems that learn from correction patterns improve accuracy over time. Manual coding quality, by contrast, tends to plateau or erode under volume pressure - which means the gap between the two widens the longer both are in use.
On the denial side, 60% of medical groups reported claim denials increased in 2024, according to an MGMA survey - and industry averages suggest nearly 60% of returned claims are never resubmitted, meaning incomplete documentation doesn't just delay revenue, it eliminates it.
KPIs impacted: Clean claim rate, denial rate, first-pass acceptance rate, days in accounts receivable, documentation completeness score
When it matters most: Multi-specialty environments, high-volume inpatient coding, organizations recovering from elevated denial rates, and health systems moving toward value-based care where documentation directly determines quality scores
Advantage 3: Compliance, Governance, and Audit Readiness
Regulatory scrutiny in healthcare is costly and growing. In FY2024, CMS program integrity activities saved $26.3 billion, with Medicare RACs identifying $486.64 million in overpayments and recovering $382.21 million of that.
HHS OCR received 30,256 HIPAA complaints in 2024, resolving 22 investigations with civil money penalties totaling nearly $10 million.
Organizations that rely on manual documentation processes face a structural disadvantage when audits arrive: records need to be located, assembled, and verified across providers, sites, and time periods - often under tight timelines.
AI-powered document analysis closes these gaps:
- Captures what was said, extracted, and decided at each step - creating a defensible audit trail without manual reconstruction
- Produces consistent documentation formats across providers, sites, and time periods so audit responses pull from structured, retrievable records rather than fragmented notes
- Enforces role-based access controls and encrypted data handling so protected health information reaches only authorized users
Cybic embeds these controls at the architecture level - RBAC, encryption in transit and at rest, audit logging, and a strict no-training-on-client-data policy are foundational to every healthcare engagement. For HIPAA alignment, that distinction is significant: controls bolted on after deployment create gaps that controls built into the architecture don't.
KPIs impacted: Audit response time, compliance incident rate, PHI breach incidents, time to produce supporting records for payer or regulatory review
When it matters most: Large health systems managing compliance across multiple sites, payer organizations handling high-volume claims review, and any organization subject to CMS, HIPAA, or Joint Commission scrutiny at scale
What Happens When AI Clinical Document Analysis Is Missing
Manual-first documentation environments consistently produce the same set of problems:
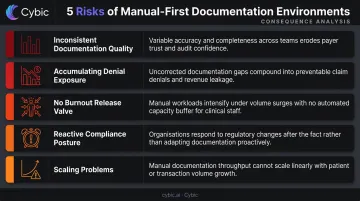
- Inconsistent documentation quality - Some providers document completely; others don't. The gap rarely surfaces until a denial or audit request makes it visible
- Accumulating denial exposure - With 60% of medical groups reporting increased denials and a large share of returned claims never resubmitted, incomplete documentation has direct revenue consequences that compound quarter over quarter
- No burnout release valve - Documentation volume grows with patient load, and manual environments have no mechanism to absorb it; providers carry the administrative overhead that automation would otherwise handle
- Reactive compliance posture - Organizations spend significant time and budget reconstructing documentation in response to audits that structured AI systems would have prepared for automatically
- Scaling problems - As patient volume grows, manual documentation overhead grows proportionally; AI document analysis breaks that linear relationship
Consider the scale gap directly: a team managing 500 encounters a month and a team managing 5,000 face identical documentation tasks per encounter. At 10x the volume, the overhead multiplies - and no amount of process improvement changes the underlying math. That's where AI document analysis changes the equation.
How to Get the Most Value from AI Clinical Document Analysis
Deployment approach determines whether AI document analysis delivers lasting improvement or stagnant output. Three principles separate the organizations that see lasting results from those that don't.
Embed AI in Existing Workflows
AI document analysis delivers operational value when it connects directly to the EHR, billing systems, and care coordination platforms. A standalone tool that requires parallel data entry or manual handoffs adds friction rather than removing it. Integration depth - not feature count - is the right evaluation criterion.
Keep Provider Review Deliberate and Structural
AI-generated notes, coding suggestions, and prior authorization drafts should be reviewed and approved by clinicians before finalization. This is both a quality and a liability requirement. The best AI systems support that review by presenting outputs in a format that makes clinician confirmation fast, not burdensome.
Track Outcomes and Act on Them
Healthcare organizations that measure documentation time, denial rates, and coding accuracy before and after deployment are the ones that identify where additional tuning is needed. Sustained improvement comes from treating AI document analysis as an evolving system - not a one-time installation. That means:
- Running governance reviews on a defined cadence
- Tracking denial rate trends against pre-deployment baselines
- Adjusting model configurations as documentation patterns shift
- Logging clinician override decisions to surface systematic gaps
Conclusion
The value of AI-powered clinical document analysis lies in consistency, accuracy, and operational control - applied across workflows that are currently expensive, error-prone, and time-consuming when managed manually. These advantages compound: reduced documentation burden frees clinical staff, improved coding accuracy protects revenue, and stronger compliance readiness reduces audit exposure. Each benefit builds on the last when AI is applied consistently under proper governance.
Healthcare organizations that implement AI document analysis as an ongoing operational capability - with governance, provider oversight, and outcome measurement built in - will outperform those that treat it as a point solution.
The documentation problem won't shrink on its own. Organizations that solve it structurally end up with more time, cleaner data, and a compliance posture they can actually defend. That's the difference between managing documentation and controlling it.
Frequently Asked Questions
What types of clinical documents can AI analyze and process?
AI systems can process a wide range of document types, including clinical notes, discharge summaries, referral letters, prior authorization requests, lab and imaging reports, and EHR data exports - both structured and unstructured. Most modern platforms handle all of these within a single processing pipeline.
How does AI clinical document analysis differ from traditional OCR or rule-based extraction?
Traditional OCR converts images to text but loses structure and clinical context in the process. AI clinical document analysis uses NLP and large language models to preserve meaning, extract relevant clinical fields, and produce structured outputs that billing, coding, and compliance systems can act on directly.
Is AI-powered clinical document analysis HIPAA compliant?
Compliance depends entirely on the platform and how it's architected. Organizations should verify that any AI document solution includes encrypted data handling, PHI de-identification, audit logging, and Business Associate Agreement (BAA) support. Compliance is not automatic and must be evaluated vendor by vendor.
How does AI document analysis help reduce physician burnout?
By automating note generation, coding suggestions, and prior authorization drafting, AI eliminates after-hours charting and repetitive data entry. One 30-day study found burnout rates dropped from 51.9% to 38.8% following ambient AI scribe adoption - documentation relief drives that result directly.
Can AI clinical document analysis integrate with existing EHR systems?
Modern AI document analysis platforms are designed for EHR integration, but the depth of that integration varies considerably. Organizations should evaluate API capabilities, workflow fit, and whether the solution connects directly within the EHR environment or requires a separate data pipeline to function.
How long does it take to see measurable results from AI clinical document analysis?
Early improvements in documentation time and claim accuracy can surface within weeks of deployment. Compounding gains in coding performance, denial reduction, and compliance readiness typically develop over several months as correction patterns accumulate and governance processes mature.