Introduction: Why Healthcare Can No Longer Afford Manual Documentation
Every day, a mid-sized hospital system processes thousands of documents - patient intake forms, prior authorization requests, insurance claims, discharge summaries, compliance reports. Most of these still move through manual workflows involving paper, re-keyed data, and human handoffs.
The numbers tell the story. The CAQH 2023 Index Report tracked 55.1 billion medical administrative transactions annually, with $18.3 billion in potential savings available if those transactions moved to fully electronic workflows. Most haven't. JAMA research estimates administrative complexity alone generates $265.6 billion in healthcare waste each year.
Document automation - shifting from paper-based, manually intensive processes to AI-powered, workflow-integrated systems - reduces errors, accelerates processing, and frees clinical and administrative staff to focus on work that actually requires human judgment.
The gap between what's possible and what most health systems are doing is where the real cost sits. This guide breaks down where that cost comes from, which document types to automate first, and what it takes to implement without disrupting the workflows your teams already depend on.
Key Takeaways
- Manual healthcare documentation drives claim denials, compliance exposure, billing delays, and staff turnover.
- Document automation eliminates redundant data entry, enforces compliance rules, and accelerates workflows from patient intake through billing.
- HIPAA-compliant security, EHR/EMR integration, AI-powered extraction, and audit traceability are must-have platform capabilities.
- Start automation with patient intake, insurance verification, prior authorizations, and consent forms - high volume, immediate impact.
- Most organizations reach ROI within 6–12 months through fewer denials, faster billing cycles, and staff redeployment.
The Real Cost of Manual Healthcare Documentation
Manual documentation isn't a minor inefficiency. It drives revenue loss, compliance exposure, and staff attrition - across the same workflows, at the same time.
Revenue and Claims Impact
Claim denials are where the financial damage is most visible. The AHA reports an average 18% in-network claim denial rate across marketplace plans, with some plans reaching 80%. When denials require rework, HFMA puts the cost at $47.77 per Medicare Advantage denial and $63.76 per commercial denial - against a backdrop of roughly 3 billion claims submitted annually.
The CAQH Index puts the processing gap in stark terms: only 28% of prior authorization transactions are fully electronic, despite electronic processing costing $5.84 versus $14.49 per manual transaction. Across millions of transactions annually, that difference is not marginal.
Compliance Exposure from Manual PHI Handling
Manual document processes create incomplete audit trails and inconsistent PHI handling - both are active enforcement targets. HHS OCR received 30,256 new HIPAA complaints in 2024 and reached 22 monetary settlements or civil monetary penalties totaling nearly $10 million in that year alone.
Enforcement cases are instructive:
- Memorial Healthcare Systems paid $5.5 million after OCR identified failures in audit controls
- MMG Fusion and TWRTC settlements both cited failures to review audit logs and information system activity records
HHS has also noted that improper disposal breaches often involve paper records placed in regular trash rather than secure shred containers - a problem automated, paperless workflows eliminate entirely.
Staff Impact
The people cost of manual documentation rarely appears in budget line items, but it shows up clearly in turnover data:
- 40% front-office support staff turnover (MGMA, 2022)
- 33.3% clinical and business operations support staff turnover (MGMA, 2022)
- A 2022 nursing study directly linked documentation burden to clinician burnout and intent to leave
The scope extends beyond attrition. A foundational Annals of Internal Medicine study found ambulatory physicians spending 49.2% of their office-day time on EHR and desk work versus 27% on direct patient care - meaning more than half the clinical workday is consumed before a patient interaction begins.

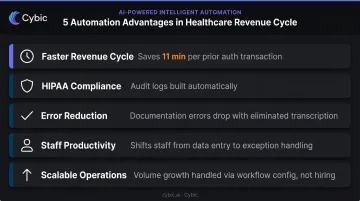
Key Benefits of Healthcare Document Automation
Faster, Cleaner Revenue Cycle Management
Automation pre-populates insurance claims from verified patient and treatment data, reducing the manual steps where errors enter. The prior authorization workflow is a clear example: CAQH data shows fully electronic processing saves 11 minutes of provider time per transaction and cuts per-transaction cost from $14.49 to $5.84, savings that compound quickly across thousands of monthly authorizations.
Electronic claim status inquiry saves an average 17 minutes per transaction compared to manual processing. When staff aren't chasing claim status by phone, they're handling exceptions, not routine lookups.
Strengthened HIPAA and Regulatory Compliance
Automated workflows embed compliance directly into the document lifecycle rather than depending on staff to follow procedures consistently. This means:
- Role-based access controls (RBAC) restrict PHI visibility to personnel who need it for their specific function
- Audit logs record every access, modification, and routing event with timestamps
- Automated compliance checks flag incomplete or non-compliant documents before they're processed or stored
- Encryption protects data both in transit and at rest
The audit trail that OCR enforcement cases consistently cite as missing gets built automatically - not as a retroactive documentation exercise.
Error Reduction at the Point of Entry
When patients enter data directly into digital intake forms that flow into EHR systems, the transcription step disappears. ECRI research found 5 in 1,000 prescriptions involved wrong-patient data entry errors. That figure drops when patient-verified data flows directly into clinical systems without manual re-entry.
A peer-reviewed study found documentation errors accounted for 23.32% of reported hospital errors. Removing the human transcription step removes the most common source of those errors.
Staff Productivity and Reallocation
Automation's biggest productivity gain is reallocation, not headcount reduction. MGMA data shows 62% of medical groups have automated 40% or less of their RCM operations, meaning most organizations are still carrying significant manual administrative load that could be redirected.
When claim status inquiries, prior authorization submissions, and insurance verification run automatically, billing staff shift from data processing to exception handling and patient financial counseling - work that delivers more value to both the organization and the patient.
Scalable Operations Without Linear Headcount Growth
Manual documentation operations require proportional staff increases as organizations face:
- Rising patient volumes
- New facilities from acquisitions
- Evolving payer requirements
Automated systems scale at the process level, handling increased volume through workflow configuration rather than hiring cycles.
Healthcare Documents That Benefit Most from Automation
Not all documents are equal candidates for early automation. The highest-impact targets share three characteristics: high volume, consistent structure, and direct connection to revenue or compliance.
Patient-Facing Clinical Documents
- Patient intake forms - auto-populated from existing records, completed digitally before arrival
- Medical histories - pulled from EHR, verified and updated by the patient without staff involvement
- Informed consent forms - routed digitally for signature, filed back to the patient record automatically
- Discharge instructions - generated from treatment data, personalized, and delivered without manual assembly
These documents touch every patient encounter. Automating them removes the manual coordination that slows each visit - gains that compound as patient volume grows.
Revenue Cycle and Insurance Documents
- Prior authorization requests - submitted electronically with supporting clinical data attached automatically
- Insurance eligibility verification - run in real time at scheduling or check-in, not manually before the appointment
- Claims submissions - pre-populated, validated for completeness before submission
- Billing statements - generated from charge data, formatted per payer requirements
Prior authorization and claims carry the largest financial stakes. Missing information, incomplete supporting documentation, and late submissions are the most common denial triggers - and automation addresses all three at the source.
Compliance and Operational Reporting
- HIPAA audit documentation - generated from system logs automatically rather than compiled manually
- Quality metrics reports (MIPS/MACRA) - drawn from live clinical data, formatted to CMS requirements; note that CMS requires performance data for at least 75% of denominator-eligible cases per measure
- Incident reports - structured, timestamped, and routed to appropriate reviewers automatically
- Accreditation records - maintained continuously rather than assembled reactively before surveys
Compliance reporting is chronically under-resourced, and manual compilation creates gaps that no amount of extra effort fully closes. Automation keeps documentation current by design, not by scramble.
Essential Features of a Healthcare Document Automation Platform
AI-Powered Data Extraction and Intelligent Document Processing
The most demanding documents in healthcare aren't structured forms - they're handwritten notes, scanned faxes, referral letters, and lab reports. AI-powered intelligent document processing (IDP) uses OCR, machine learning, and natural language processing to convert these unstructured inputs into structured EHR data.
The practical capability this enables: a scanned referral letter arrives, the system extracts patient identifiers, diagnosis codes, and requested services, routes the information to the correct clinical and scheduling workflows, and creates the necessary documentation - without a staff member manually reading and re-keying the document.
Cybic's governed AI automation platform combines IDP with embedded auditability, traceability, and a strict no-training policy on proprietary enterprise data - meaning patient records and clinical documents process through the system without being incorporated into any model training datasets.
HIPAA-Compliant Security Architecture
The security layers that matter:
| Security Component | What It Does | What Its Absence Creates |
|---|---|---|
| End-to-end encryption | Protects PHI in transit and at rest | Breach exposure at every transfer point |
| Role-based access controls | Limits PHI visibility by job function | Unauthorized access that triggers HIPAA violations |
| Multi-factor authentication | Verifies identity before system access | Credential-based intrusions |
| Automatic session timeouts | Closes active sessions on idle workstations | Unattended access to open patient records |
| Immutable audit logs | Records every access and modification | No audit trail for compliance investigations |
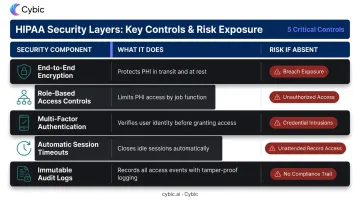
Each layer maps to a specific enforcement pattern in HHS Office for Civil Rights settlement history. Together, they make HIPAA compliance something the system enforces continuously - not something the compliance team reconstructs after the fact.
Seamless EHR/EMR and Healthcare System Integration
True integration means data entered once flows bidirectionally to all relevant systems: EHR, practice management, billing, lab information, and scheduling. A platform that merely centralizes document storage without connecting to downstream systems just relocates the problem.
This requires genuine API-based integration with existing systems, not manual exports and imports relabeled as integration. Cybic's AI and data ecosystem integration capability connects automation platforms to existing clinical and operational infrastructure, enabling data exchange across systems without re-entry.
Configurable Workflow Builder
Regulatory requirements change. Payer documentation standards shift. New service lines launch. Clinical, billing, and compliance teams need to adapt workflows without waiting for IT development cycles. A configurable, low-code workflow builder gives operational teams direct control - without developer involvement - over:
- Document routing rules based on document type, department, or extracted data values
- Validation checkpoints that flag missing fields or non-compliant entries before submission
- Approval chains for prior authorizations, referrals, and compliance sign-offs
Infrastructure Flexibility
Health systems managing multi-site operations or acquisition-driven growth can't afford to be locked into a single infrastructure model. The right platform runs across cloud (AWS, Azure, GCP), hybrid, and on-premises environments. Cybic's architecture is explicitly infrastructure-agnostic, designed for organizations operating across diverse and evolving infrastructure footprints.
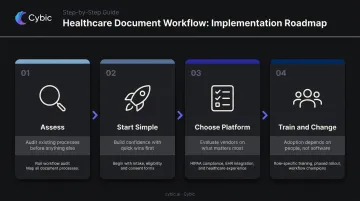
Implementing Document Automation in Healthcare: A Step-by-Step Approach
Step 1: Assess Before You Automate
Run a workflow audit before selecting any technology. Map every document process from patient registration through billing and compliance reporting. For each process, capture:
- Time per step
- Volume per day/week/month
- Error rate and rework frequency
- Compliance sensitivity (does it involve PHI, billing, or regulatory reporting?)
This baseline does two things: it tells you where automation will deliver the highest return, and it gives you the measurement foundation to demonstrate ROI post-implementation.
Step 2: Start with High-Impact, Lower-Complexity Documents
Patient intake, insurance eligibility verification, and consent management are the right starting points. They touch every patient, produce immediate throughput gains, and don't require complex clinical decision logic. Early wins here also build staff confidence and reduce resistance when it's time to tackle more complex clinical workflow automation.
Step 3: Choose the Right Platform and Implementation Partner
Evaluate vendors on healthcare-specific criteria:
- Pre-built HIPAA compliance - not a configuration option, a default
- EHR integration depth - bidirectional, API-based, with named systems they've connected to
- Prior healthcare implementation experience - ask for specifics, not general claims
- Engineering-led delivery - the people who design the solution should build it
Cybic applies this last criterion directly: the same engineers who scope the compliance requirements and integration constraints are the ones who build and deploy the system, eliminating the handoff gaps that slow most implementations.
Step 4: Train Staff and Manage the Change
Automation deployments stall on adoption, not technology. A practical change management framework:
- Role-specific training - clinical, administrative, and billing teams have different workflows and concerns; train them separately
- Phased rollout - start with one or two pilot departments before organization-wide deployment
- Workflow champions - designate staff who become the internal experts and first line of support
- Communicate wins early - publish the reduction in claim denial rate or intake time saved in the first 60 days; concrete numbers sustain momentum better than general messaging
Frequently Asked Questions
What types of healthcare documents can be automated?
Common candidates include:
- Patient intake and consent forms
- Insurance eligibility checks and prior authorization requests
- Claims submissions and billing statements
- Compliance and quality reports
- Discharge instructions and lab requisitions
- Explanation of benefits documents
Any document that requires consistent formatting and draws data from electronic systems is a strong candidate.
How does document automation support HIPAA compliance?
Automation enforces compliance through built-in RBAC, encrypted data storage and transmission, comprehensive audit logs tracking who accessed what and when, and automated checks that flag non-compliant documents before processing. Compliance is embedded in the architecture, not left to manual processes.
How does document automation integrate with EHR and EMR systems?
Modern platforms integrate in both directions with major EHR/EMR systems using APIs and pre-built connectors. Data entered once - at intake, during a visit, or in billing - flows across clinical, scheduling, billing, and lab systems without manual re-entry.
What is the typical ROI timeline for healthcare document automation?
Most organizations see measurable returns within 6–12 months, with early gains in reduced denial rates and processing times. Longer-term returns come from staff reallocation, faster billing cycles, and lower compliance risk.
How is AI-powered document automation different from traditional automation?
Traditional automation handles structured, predictable documents using rule-based logic. AI-powered automation uses machine learning and NLP to process unstructured inputs - handwritten notes, scanned faxes, referral letters - and improves accuracy over time without manual reprogramming.
What should healthcare organizations prioritize when selecting a solution?
Prioritize HIPAA-compliant security architecture, proven EHR/EMR integration, AI-powered data extraction, infrastructure flexibility, and a vendor with demonstrated healthcare experience who can deliver working systems - not just recommendations.