Introduction: The Hidden Cost of Healthcare Administration
Healthcare organizations face a persistent financial drain that has nothing to do with patient care. According to JAMA research, administrative expenses consume 15% to 25% of total US healthcare expenditures - roughly $600 billion to $1 trillion annually. With US healthcare spending hitting $5.3 trillion in 2024, even modest efficiency gains translate into enormous dollar impact.
The back-office machinery - billing, coding, claims, scheduling, credentialing, compliance - absorbs resources without generating direct care value. Staff spend hours on repetitive data entry, phone-based claim follow-up, and manual eligibility checks.
CAQH estimates these administrative transactions cost roughly $90 billion annually, with full electronic automation potentially saving $20 billion more and 70 minutes per patient visit.
AI agents are now doing the work that previously required full-time staff: reasoning over context, executing multi-step workflows, and handling exceptions without requiring human intervention at every turn. These are not chatbots or simple rule-based scripts.
This guide covers where these agents operate, what they actually do, and what healthcare organizations need to know before deploying them.
Key Takeaways
- Administrative costs consume 15–25% of US healthcare spending - back-office automation directly attacks this burden
- AI agents outperform RPA by handling exceptions and variable workflows, not by following rigid scripts
- Highest-ROI starting points: eligibility verification, claim follow-up, coding, and appointment reminders
- HIPAA compliance demands BAAs, encryption, RBAC, audit trails, and a strict no-PHI-for-model-training policy
- ROI compounds over time: documented results include denial reductions, faster A/R cycles, and measurable FTE redeployment
What Are AI Agents for Healthcare Back-Office?
Defining the Category
Back-office AI agents are autonomous software systems that handle the operational machinery of healthcare - not clinical decisions, but the workflows that surround them. Billing, claims, coding, scheduling, credentialing, compliance tracking. They execute sequential tasks across connected systems without requiring a human to trigger each step.
The distinction from clinical AI matters. A clinical AI might flag a diagnostic anomaly. A back-office AI agent submits a clean claim, follows up on its status five days later, and escalates a denial risk before submission. No scheduler or billing coordinator needs to initiate any of it.
Why AI Agents Beat RPA Here
Traditional robotic process automation follows pre-defined scripts. When a system interface changes, a field moves, or an exception arises that wasn't anticipated during the build, the bot fails. Healthcare back-office environments are exactly the kind of high-variance, high-exception workload that breaks RPA.
AI agents operate differently:
- Interpret context, not just screen coordinates
- Handle exceptions by reasoning over the situation, not stopping cold
- Adapt to variability in payer rules, documentation formats, and workflow states
- Make conditional decisions without a human writing every rule in advance
A healthcare RPA review published in PMC identified integration complexity, data-quality dependence, and operational difficulty under high volumes as core limitations of rule-based automation - limitations that agents are specifically designed to overcome.
Supervised Autonomy in Practice
Current healthcare back-office deployments don't operate without oversight. The appropriate model is supervised autonomy: agents handle the execution work while humans focus on flagged exceptions and high-risk decisions rather than approving every routine action.
In practice, that split looks like this:
- Agents handle: data extraction, validation, claim submission, and status tracking
- Humans review: flagged exceptions, denial escalations, and high-risk edge cases
This division is both practical and necessary given the financial and regulatory stakes involved.
Key Back-Office Functions AI Agents Are Automating
Revenue Cycle Management and Claims Processing
End-to-end RCM is where back-office AI agents produce the clearest measurable ROI. A capable agent handles:
- Pre-visit insurance eligibility verification against payer databases
- Real-time procedure code suggestions aligned with clinical documentation
- Clean claim construction and submission
- Automated follow-up on pending claims at defined intervals
- Denial prediction before submission, flagging claims likely to be rejected based on payer-specific rules and historical patterns
That last capability is what separates AI agents from traditional billing software. Rather than managing denials after the fact, agents identify risk proactively, giving staff a window to intervene before a claim is ever submitted.
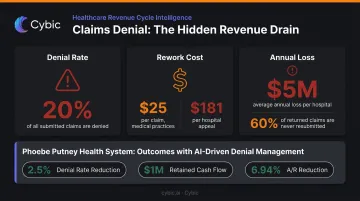
AHIMA reports nearly 20% of claims are denied, with rework costing $25 per claim for a medical practice and $181 for a hospital appeal. Unresolved denials average $5 million in annual losses for hospitals, and as many as 60% of returned claims are never resubmitted at all.
Phoebe Putney Health System reported a 2.5% denial-rate reduction, 1.1% underpayment reduction, nearly $1 million in retained net cash, and a 6.94% reduction in A/R over 90 days after deploying AI-driven denial analytics.
Medical Coding and Clinical Documentation
AI coding agents ingest clinical notes, physician dictation, and visit summaries, then autonomously suggest ICD-10, CPT, and HCC codes aligned with payer guidelines. Voice-to-action functionality translates physician speech directly into structured documentation, cutting manual entry time for clinicians while improving coding accuracy.
The financial stakes here are significant. CMS reported $31.70 billion in Medicare fee-for-service improper payments in FY2024 - with insufficient documentation driving the majority of Medicaid improper payments. Undercoding and overcoding both carry real costs: undercoding leaves revenue on the table, overcoding creates compliance exposure.
At Mass General Brigham, contextual coding automation from CodaMetrix delivered nearly a 60% reduction in coding-related denials.
Scheduling and Patient Access Administration
Scheduling agents manage the full appointment lifecycle autonomously:
- Slot matching based on provider availability, patient need, and insurance requirements
- Automated reminders via patient-preferred channels
- Rescheduling triggered by cancellations without staff involvement
- Pre-registration data collection pushed directly into the EHR
North Kansas City Hospital and Meritas Health deployed Notable Health's AI platform and reported a 90%+ reduction in check-in time, 80 open roles that did not need to be filled, and a 34% decrease in no-shows - numbers that translate directly into capacity recovery during a period when administrative hiring remains difficult across health systems.
Compliance Monitoring and Supply Chain
Compliance agents continuously scan for documentation gaps, unusual data access patterns, and regulatory changes - without waiting for a scheduled audit. Every agent action generates a structured log, creating an audit trail that supports HIPAA compliance and prepares organizations for CMS and payer reviews.
Supply chain and credentialing agents handle two areas that rarely get attention but consistently deliver value:
- Matching supply orders to inventory consumption patterns to reduce waste and shortages
- Tracking provider license renewals and credentialing expiration dates automatically
- Automating HR tasks like onboarding paperwork and benefits queries
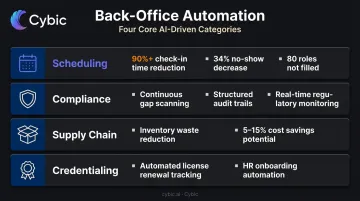
McKinsey estimates health systems can capture 5% to 15% cost savings from external spend optimization. Supply chain automation accounts for a significant share of that figure.
Benefits of AI Agents in Healthcare Back-Office Operations
Benefits fall into two categories: financial and operational. Both grow more pronounced as agents improve through feedback cycles over time.
Faster Revenue Capture and Reduced Billing Errors
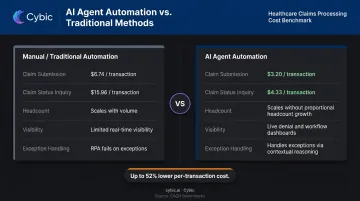
Automated eligibility checks, clean claim submission, and proactive denial management compress the revenue cycle directly. CAQH benchmarks show manual claim submission costs $6.74 per transaction versus $3.20 electronically - and manual claim status inquiries cost $15.96 versus $4.33 electronically. At high volume, those per-transaction gaps add up fast.
HFMA's 2024 MAP Award data shows top-performing health systems carrying net days in A/R at 38.3 days at median. Reducing that by even a few days has significant working-capital implications for large systems.
Staff Redeployment and Burnout Reduction
AI agents don't eliminate administrative jobs - they change what those jobs involve. Staff shift from repetitive data entry and phone-based claim follow-up to exception handling, patient communication, and higher-value coordination work.
Administrative burnout is well-documented: an MGMA poll found 8 in 10 medical group practice leaders reported increased stress and burnout in 2022, with payer challenges and prior authorization at the top of the list. Removing high-volume repetitive tasks reduces that pressure at the source - and frees budget. In one health system deployment, AI agents absorbed enough workflow volume that 80 open roles never needed to be filled, eliminating both hiring costs and onboarding overhead.
Scalability and Operational Visibility
Two operational advantages set AI agents apart from conventional automation:
- Scalability without proportional cost growth. When patient volume increases or an organization absorbs an acquisition, AI agents handle the additional load without requiring proportional headcount growth - a direct advantage for growing health systems and multi-site practices.
- Real-time operational visibility. Agents generate structured data as they work - every claim status, scheduling action, and compliance flag. Administrators and CFOs gain live visibility into denial trends, workflow bottlenecks, and performance metrics that previously required manual reporting pulls.
How Healthcare Back-Office AI Agents Actually Work
Data Ingestion and System Integration
Back-office AI agents work by connecting to existing healthcare systems - EHRs, practice management platforms, billing systems, payer portals - via FHIR/HL7 APIs and secure connectors. ONC identifies HL7 FHIR as the primary standard for API-based health information exchange, with the Cures Act Final Rule establishing standardized API requirements across certified health IT systems.
The agent reads both structured data (insurance records, claim status, scheduling slots) and unstructured data (clinical notes, EOBs, physician dictation) to build context before acting.
Integration depth is the single biggest variable in deployment complexity. Organizations should prioritize vendors with pre-built connectors for their specific EHR and billing platform to reduce custom development time.
Platforms like Cybic's Drava are designed to connect enterprise data, machine learning, and intelligent agents into unified operational systems - the architecture that makes multi-system healthcare workflows manageable rather than a custom build for each integration.
Reasoning, Decision-Making, and Task Execution
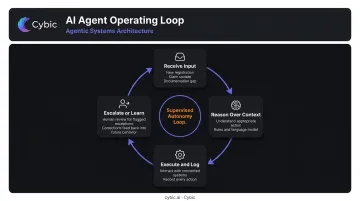
The agent's operating loop:
- Receive input - a new patient registration, a claim status update, a flagged documentation gap
- Reason over context - using an LLM or rules engine to understand what action is appropriate
- Select and execute - interact with one or more connected systems
- Log the action - record what was accessed, what was decided, what was changed
Concrete example: an agent receives a new patient registration, queries a payer API to verify insurance eligibility, identifies a coverage gap, updates the patient record in the EHR, and creates a task in the billing queue. No human initiates the sequence.
Human-in-the-Loop Escalation and Continuous Learning
When confidence falls below a threshold, a well-designed agent escalates to a human reviewer with full context attached. Triggers include complex multi-payer claims, compliance edge cases, and coding decisions with ambiguous documentation. The escalation package includes:
- The supporting data and relevant claim or coding context
- The agent's reasoning and confidence level
- Available resolution options for the reviewer
This supervised autonomy model is non-negotiable in healthcare back-office specifically. Errors carry financial consequences (denied claims, underpayments) and regulatory exposure (audit findings, OIG scrutiny). The goal is to minimize human review to the decisions that require judgment, not to automate everything unconditionally.
Those correction points also drive improvement. When a human overrides a coding suggestion, approves an escalated claim, or adjusts a scheduling decision, that signal feeds back into future agent behavior. In high-volume environments, a 1% accuracy improvement across millions of claims translates to material cost savings - which is why this learning loop matters as much as the initial deployment.
Governance, Compliance, and Security Considerations
In healthcare back-office AI, security and compliance must be built into the architecture from day one. Every agent action touches PHI - and the design choices made upfront determine whether your system holds up under audit.
HIPAA Requirements That Apply Directly
| Requirement | Regulation | What It Means for AI Agents |
|---|---|---|
| Administrative safeguards & BAAs | 45 CFR 164.308 | Vendors processing PHI must sign a Business Associate Agreement |
| Audit controls | 45 CFR 164.312(b) | Every agent action touching ePHI must be logged and examinable |
| Encryption | 45 CFR 164.312(a)(2)(iv) | PHI must be encrypted in transit and at rest |
| Minimum necessary access | 45 CFR 164.502(b), 164.514(d) | Agents should only access PHI required for the specific task |
The minimum necessary principle has direct implications for agent design: an agent handling eligibility verification has no business accessing clinical documentation outside that workflow.
Auditability, RBAC, and Vendor Evaluation
Role-based access controls and full audit trails are the mechanism by which organizations prove what happened during an audit. Every agent action needs to be traceable - what data was accessed, what decision was made, what system was updated, and when.
Bolt-on compliance tools frequently create gaps that surface during actual audits. Cybic builds RBAC, encrypted data protection, and AI action auditability into the architecture from the start - and explicitly prohibits model training on proprietary enterprise data, a policy that affects which vendors can safely handle your PHI.
Questions to ask any back-office AI vendor:
- Does the vendor sign a BAA?
- Is the infrastructure SOC 2 Type II certified?
- Where is PHI processed and stored - cloud, hybrid, or on-prem?
- Does the vendor train models on your proprietary patient data?
- What triggers human escalation for high-risk decisions?
- How are audit logs structured and made available for HIPAA or payer audits?
Frequently Asked Questions
What is the difference between AI agents and RPA in healthcare back-office?
RPA follows rigid, pre-defined scripts and fails when system interfaces change or exceptions arise outside the original design. AI agents reason over context, handle unexpected situations, and adapt to variable inputs - making them better suited to healthcare billing and compliance workflows, where payer rules, documentation formats, and claim statuses vary constantly.
Which back-office processes should be automated with AI agents first?
Start with high-volume, rule-heavy workflows where errors are measurable and ROI is clear: insurance eligibility verification, claim status follow-up, appointment reminders, and denial flagging. These deliver fast time-to-value and build the organizational confidence needed to justify broader rollout.
How do AI agents maintain HIPAA compliance in healthcare back-office?
Five requirements are non-negotiable:
- End-to-end PHI encryption in transit and at rest
- Role-based access controls limiting data exposure per task
- Full audit trails of every agent action
- Signed BAAs with all vendors processing PHI
- No use of patient data to train external models
Can AI agents integrate with existing EHR and billing systems?
Yes. Modern AI agent platforms integrate via FHIR/HL7 APIs and vendor-specific connectors. Organizations should prioritize vendors with pre-built connectors for their specific EHR and billing platform - this directly reduces deployment time and custom development costs.
How long does implementation typically take?
Targeted automations - eligibility verification, appointment reminders, claim status follow-up - can go live in weeks. Enterprise-wide back-office agent deployments typically require 3–6 months to reach full production, depending on integration complexity and the number of connected systems.
What ROI can healthcare organizations realistically expect?
Published case studies provide the most reliable benchmarks: Phoebe Putney reported a 2.5% denial-rate reduction and nearly $1 million in retained net cash; Mass General Brigham cut coding-related denials by nearly 60%; NKCH avoided filling 80 open roles. Organizations that commit to multi-workflow deployments - rather than single-task pilots - consistently see the strongest returns.