Introduction
Healthcare has spent decades trailing other industries on technology adoption. That era is ending - driven not by a sudden appetite for technology, but by economics that left no other choice.
Hospital margins sat at just 2.3% in 2023, with 40% of hospitals operating in the red, according to Kaufman Hall. The AAMC projects a shortage of up to 86,000 physicians by 2036. Administrative burden consumes clinician time that patients need. These pressures don't respond to incremental fixes.
AI adoption in healthcare has accelerated sharply in response. The ONC reported that 71% of hospitals used predictive AI integrated with EHRs in 2024, up from 66% the year before. That's a meaningful single-year jump for an industry that took over a decade to adopt electronic health records.
This article covers what's driving that acceleration, which use cases are delivering results, and what's preventing most pilots from reaching production. It closes with a practical implementation framework for organizations ready to move past experimentation.
Key Takeaways
- 71% of hospitals now use predictive AI integrated with EHRs - adoption is real and accelerating
- Highest-ROI use cases: clinical documentation, imaging diagnostics, sepsis prediction, and billing automation
- AI's biggest promise is recovering clinician time - physicians currently spend nearly half their office hours on administrative tasks
- Most pilots stall due to governance gaps, fragmented data, and integration complexity - not budget shortfalls
- Successful implementation starts with governance infrastructure, production-ready pilots, and a real change management plan
Why Healthcare Is at an AI Inflection Point Right Now
Healthcare organizations are under pressure from three directions at once - and none of them are letting up.
Margin pressure is severe. With a median hospital operating margin of 2.3% and four in ten hospitals losing money, there's no financial slack to absorb inefficiency. Every hour of wasted clinical time and every preventable readmission carries real cost.
The workforce shortage is structural, not cyclical. HRSA projects an 81,180 FTE physician shortage by 2035, with demand outpacing projected supply by roughly 80,000 physicians. No hiring strategy closes that gap. Productivity tools aren't optional - they're arithmetic.
Patient expectations have shifted. Consumer-grade digital experiences have reset what patients expect from healthcare interactions. Organizations that can't deliver responsive, personalized, digitally-enabled care face real competitive disadvantage.
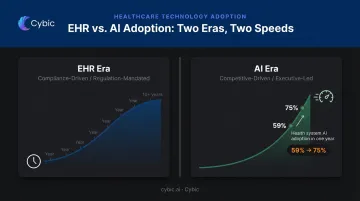
AI Adoption Is Moving on a Different Timeline Than EHR Did
The EHR era was compliance-driven - government-incentivized, regulation-mandated, and slow. It took more than a decade to reach meaningful adoption.
AI adoption is moving faster because the driver is competitive pressure, not regulatory mandate. It's executive-led, decentralized, and accelerating. 75% of U.S. health systems used at least one AI application in 2026, up from 59% the prior year, with 50% using three or more applications. That jump in a single year reflects organizations making active strategic choices, not checking compliance boxes.
Key AI Use Cases in Healthcare Today
Clinical Documentation and Ambient AI Scribes
Documentation burden is one of the most corrosive forces in clinical medicine. Physicians spend nearly half their office hours on EHR and desk work. For every hour of direct patient contact, they log close to two additional hours of documentation - and that's before after-hours charting.
Ambient AI documentation tools address this directly. These systems listen to patient-provider conversations and automatically generate structured clinical notes, without requiring physicians to manage a keyboard during the visit.
Early deployment data shows measurable impact:
- Microsoft DAX Copilot: Saved an average of 5 minutes per encounter across a survey of 879 clinicians (vendor-reported)
- Abridge: Deployed across 150+ enterprise health systems, on track to support 50 million clinical conversations in 2025
The numbers are vendor-reported, but deployment at that scale reflects real clinical uptake - not just pilot programs.
Diagnostics, Imaging, and Predictive Analytics
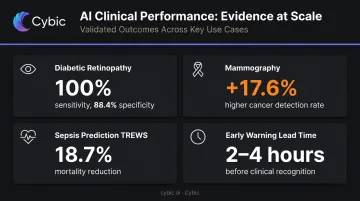
AI's diagnostic performance in specific imaging tasks now matches or exceeds specialist-level accuracy in controlled settings:
- Diabetic retinopathy screening: AI achieved 100% sensitivity and 88.4% specificity for referable cases in peer-reviewed JAMA Ophthalmology research
- Mammography: A large-scale real-world implementation found AI-supported screening detected breast cancer at a rate 17.6% higher than control groups
- Sepsis prediction: The TREWS system, studied across 590,736 patients at five hospitals, was associated with an 18.7% adjusted reduction in in-hospital mortality when alerts were confirmed within three hours
- Early warning lead time: Most ML-based sepsis tools surface alerts two to four hours before clinical recognition - a window that directly affects survival outcomes
Operational and Revenue Cycle Automation
Administrative and revenue cycle automation tends to deliver measurable ROI faster than clinical AI - making it a practical starting point for health systems building their AI programs:
- Predictive AI use for billing automation jumped from 36% to 61% of hospitals in a single year (2023 to 2024)
- Electronic prior authorization adoption could save an estimated $515M annually and 14 minutes per authorization, per CAQH analysis
- Medical coding, claims processing, staff scheduling, and supply chain management are all active deployment areas with measurable ROI potential
The Real Benefits of AI Adoption in Healthcare
Clinical Benefits: Better Decisions, Earlier Interventions
AI's clinical value is built on pattern recognition at scale. No individual clinician can process population-level data in real time. AI can - and in high-acuity settings like ICUs and emergency departments, that speed advantage directly affects survival rates.
The sepsis example is instructive. Getting a warning two to four hours earlier than conventional clinical recognition allows targeted intervention before cascading organ failure begins. The TREWS mortality reduction data reflects that reality.
Beyond acute care, AI is advancing personalized medicine. By integrating genomic data, longitudinal EHR history, and real-time wearable inputs, AI models can predict individual patient responses to specific drugs or therapies.
That shifts prescribing from population-level averages toward genuinely individualized treatment, reducing adverse drug reactions and improving outcomes for patients who would otherwise receive standard-of-care protocols that weren't designed for them.
Operational and Financial Benefits
The administrative burden data is striking. Research published in the Annals of Internal Medicine found ambulatory physicians spent 49.2% of office time on EHR and desk work versus just 27% on direct clinical face time. That inversion is not sustainable, and it's a direct contributor to burnout.
AI-powered automation of documentation, coding, and administrative workflows directly reclaims that time. The downstream effect isn't just efficiency - retention follows. Burned-out physicians leave, and replacing one costs hundreds of thousands of dollars over years. Preventing that attrition through workload reduction carries significant financial value that rarely appears in ROI models.
At the system level, McKinsey projects that AI, traditional machine learning, and deep learning could generate $200B to $360B in net healthcare spending savings annually. That figure includes reduced readmissions, fewer diagnostic errors, optimized workforce allocation, and revenue from personalized services - positioning AI as a revenue driver, not just a cost-reduction lever.
Workforce Resilience
The physician shortage cannot be solved by hiring alone. AI addresses the structural gap by amplifying clinician capacity rather than replacing it:
- Real-time patient monitoring frees nurses from constant manual checks
- Automated scheduling reduces administrative load on care coordinators
- Triage support tools help emergency departments manage higher volumes without proportional staffing increases
Taken together, these capabilities let health systems expand patient throughput without a proportional increase in headcount - a critical equation as workforce shortages deepen across the US.
The Barriers Holding AI Back: Why Most Pilots Never Scale
Many health systems have launched AI pilots. Far fewer have moved them to production. The gap is between a controlled experiment and a system that actually runs inside clinical workflows - handling compliance requirements, legacy integrations, and skeptical end users simultaneously.
Data Readiness and Integration Complexity
Fragmented data is the most fundamental barrier. Healthcare data lives across legacy EHRs, claims systems, lab platforms, payer databases, and an expanding ecosystem of wearable devices - rarely in formats that AI models can consume directly.
What "AI-ready data" actually requires:
- Clean, consistent pipelines with standardized data formats across source systems
- Data governance policies covering ownership, access, lineage, and quality standards
- Interoperability infrastructure that most health systems have not yet fully built
- Integration with legacy EHR platforms - which is expensive, technically complex, and time-consuming, particularly for large payers with entrenched legacy architectures
Underestimating integration scope is one of the most common reasons implementations stall after a promising pilot.
Security, Compliance, and Governance Gaps
The regulatory surface in healthcare is unforgiving. 386 healthcare cyberattacks were reported in the first nine months of 2024 alone, according to the AHA - and every new AI integration expands the attack surface.
HIPAA-mandated data protection, auditability of AI-driven clinical decisions, and strict policies ensuring patient data is never used to train external models aren't optional compliance checkboxes. They're architectural requirements. Organizations that bolt governance on after deployment rather than building it in from the start face disproportionate regulatory and reputational exposure.
This is where architectural approach matters. Cybic designs governance, RBAC, auditability, and HIPAA alignment directly into its AI solutions from day one - treating compliance as an engineering constraint built into the system, not a review process appended at the end.
Algorithmic Bias and Explainability
Data and governance infrastructure are only part of the picture. Even well-integrated AI can fail patients if the underlying models are flawed or opaque.
A landmark study published in Science found that a widely used population health algorithm - affecting millions of patients - exhibited significant racial bias. Correcting it would have increased Black patients identified for additional care from 17.7% to 46.5%. That's a systematic failure embedded in a production system, not an edge case.
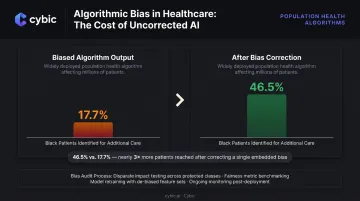
Two distinct problems drive this. Models built on historically unrepresentative datasets replicate - and can amplify - existing care disparities. Separately, clinicians cannot act confidently on recommendations they cannot interpret, and regulators increasingly require explainability before approving clinical AI tools for deployment.
Addressing both requires proactive bias auditing during model development and architectures designed to surface reasoning alongside outputs - before clinical users ever see a recommendation.
A Practical Framework for Healthcare AI Implementation
Phase 1: Build Governance and Data Infrastructure First
The most common implementation mistake is selecting a tool before the foundation is ready.
Before any model is deployed, organizations should:
- Audit existing data assets - understand what data exists, where it lives, and what state it's in
- Establish data governance policies (access controls, data lineage, compliance alignment, ownership definitions)
- Map clinical and operational workflows to understand how AI fits into existing processes before designing around them
- Define production-readiness criteria (what success looks like, and what the system must do before going live)
On use case selection: start with high-frequency, lower-risk workflows where ROI is measurable and stakeholder resistance is lower. Clinical documentation, coding automation, and scheduling are natural starting points. Avoid launching with high-stakes clinical decision support as a first initiative - build credibility before raising the stakes.
Phase 2: Design the Pilot to Survive the Move to Production
Most pilots are designed to succeed in isolation. Production systems need to succeed in the real world.
A pilot built to scale shares several characteristics that distinguish it from a proof-of-concept that never survives deployment:
- Defines success metrics upfront - financial (cost savings, revenue impact) and operational (clinician time recovered, error reduction, adoption rates)
- Involves legal, IT, security, and compliance teams from the start, not as final-stage reviewers
- Sets explicit production-readiness criteria before the first line of code is written
- Tests under real workflow conditions, not controlled demo environments
The real question isn't whether the pilot worked. It's whether the pilot proved the system can perform at scale, under real conditions, within compliance boundaries.
Phase 3: Treat Adoption as a People Problem
Technology implementation is the easier half. The harder half is getting clinicians and staff to trust, use, and benefit from the system.
The most overlooked implementation risk is internal resistance from clinicians skeptical of disruption, managers uncertain about accountability, and end users who weren't part of the selection process and feel like AI is being done to them rather than for them.
Effective change management in healthcare AI includes:
- Executive storytelling that connects AI deployment to organizational mission, not just efficiency metrics
- Super-user programs that identify clinical champions early and train them before broad rollout
- Transparent communication about what AI handles and what remains a human decision
- Rapid iteration based on frontline feedback - the system should adapt to users, not just the other way around

Post-deployment, the work continues. AI systems require ongoing monitoring for performance drift, bias, and security gaps. Audit trails of AI-driven decisions must be maintained for regulatory and accountability purposes. Cybic structures this into every healthcare engagement: auditability and traceability are built into the architecture from day one, and proprietary patient data is never used to train models - because governance that gets added after deployment rarely holds.
Frequently Asked Questions
What are the most common AI use cases in healthcare right now?
The most widely deployed use cases include:
- Ambient clinical documentation (AI scribes)
- Medical imaging diagnostics
- Predictive risk stratification (sepsis, readmission)
- Medical coding and billing automation
- Patient engagement tools and prior authorization automation
What is the biggest barrier to scaling AI in healthcare?
Data readiness is the primary barrier: most health systems have fragmented data across legacy systems that isn't AI-ready. Security and compliance gaps, combined with a shortage of in-house AI expertise, make moving pilots into production significantly harder.
Will AI replace doctors and nurses in healthcare?
AI is designed to augment clinicians, not replace them. It handles documentation, administrative tasks, and repetitive analytical work so care teams can focus on patients and complex decisions. Given the ongoing physician shortage, amplifying clinical capacity is the goal - not reducing headcount.
How long does it take to implement AI in a healthcare organization?
Procurement timelines have compressed significantly, but full production deployment - including EHR integration, compliance validation, and staff adoption - typically spans 12–18 months depending on use case complexity and organizational readiness.
How does healthcare AI handle patient data privacy and HIPAA compliance?
Compliant systems require encryption in transit and at rest, role-based access controls, full audit trails, and HIPAA-aligned data governance. The most critical requirement: patient data must never be used to train external AI models - and that protection needs to be enforced at the architectural level, not just written into contracts.
What ROI can healthcare organizations realistically expect from AI adoption?
McKinsey projects AI could generate $200B to $360B in annual net healthcare savings from reduced errors, lower readmissions, workforce optimization, and new revenue streams. Administrative and revenue cycle use cases tend to show measurable financial impact earliest. ROI should be tracked across both financial metrics (cost savings, revenue) and operational ones (clinician time recovered, error reduction rates).