Introduction
US healthcare spending hit $5.3 trillion in 2024 - 18% of GDP - yet a substantial portion of that money funds paperwork, not patient care. According to Health Affairs, administrative spending accounts for 15–30% of total health expenditures, with at least half of that considered wasteful.
Most hospitals have had EHRs for years. Yet having digital records doesn't mean having automated workflows. Manual handoffs, disconnected systems, and repetitive data-entry tasks still consume enormous amounts of clinical and administrative time - costs that compound quickly at scale.
This article walks through how to systematically identify which workflows are ready for automation, where to start, and what governance foundations you need before deploying anything.
Key Takeaways
- Focus on workflows that are high-volume, rule-based, repetitive, and error-prone - they offer the clearest path to measurable impact
- Prior authorization, claims processing, eligibility verification, appointment reminders, and care coordination are top automation candidates with strong ROI potential
- Rank candidates by patient impact, cost savings, staff burden, and integration complexity
- Map your current-state processes before selecting tools - automating a broken process just breaks it faster
- HIPAA compliance and data governance must be built into the architecture, not bolted on afterward
Why Healthcare Workflows Are Overdue for Automation
Physicians spend roughly 49% of their office day on EHR and desk work compared to only 27% on direct patient face time, according to a widely cited AHA-reported study. The time gap isn't incidental - it's the direct result of workflows built around documentation requirements rather than clinical priorities.
The administrative burden creates compounding downstream effects:
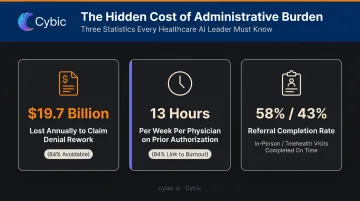
- $19.7 billion lost annually to claim denial review and rework - with 84% of those denials potentially avoidable
- 13 hours per week consumed per physician on prior authorization alone - 94% of physicians link it directly to burnout, per the 2025 AMA Prior Authorization Survey
- Recommended tests and referrals completed on time for only 58% of in-person visits and 43% of telehealth visits, per a 2023 JAMA Network Open study - a patient safety gap, not just an efficiency one
A common response to this data is that EHR adoption has already solved the problem. It hasn't. While 96% of acute care hospitals have certified EHRs, only 43% routinely engage in all four interoperability domains, per a 2024 ONC data brief. Having a digital record system and actually closing the loop on information exchange remain two separate achievements.
The Diagnostic Framework: 5 Signs a Workflow Is Ready for Automation
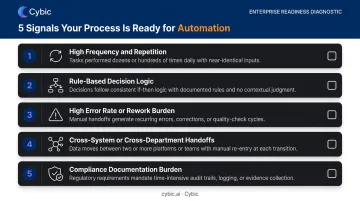
Before you select a platform or build a business case, you need a way to screen workflows. Here are five reliable signals:
Signal 1: High Frequency and Repetition
Tasks performed dozens or hundreds of times daily - appointment reminders, eligibility checks, lab result routing - are strong candidates. Frequency multiplies both time cost and error rate. A 2% error rate on 500 daily transactions is 10 errors per day; on 5,000, it's 100.
Signal 2: Rule-Based Decision Logic
Workflows governed by clear "if-then" logic (claim scrubbing, referral routing, discharge checklists) can be reliably automated without complex AI. The key distinction: rule-based logic is automatable; nuanced clinical judgment requires human oversight. Treating them as equivalent leads to automation projects that fail compliance review or produce unsafe outputs.
Signal 3: High Error Rate or Rework Burden
Track rework volume directly. The Optum 2024 Denials Index found the average hospital claim denial rate reached 12% in 2023, up from 9% in 2016, with registration and eligibility issues causing 24% of those denials. Where error rates are climbing, manual processes are breaking down.
Signal 4: Cross-System or Cross-Department Handoffs
Any workflow that requires passing information between EHR, LIS, billing, radiology, pharmacy, and the front desk is a risk point. Each handoff introduces delay and a new opportunity for data to be lost, duplicated, or miscommunicated. Studies consistently show that handoff failures contribute to a significant share of adverse events - and these are exactly the gaps automated orchestration is designed to close.
Signal 5: Compliance Documentation Burden
Processes that require an audit trail - medication administration records, PHI access logs, prior authorization records - benefit directly from automation. When a system executes the process, documentation becomes a byproduct of execution rather than a separate manual step.
Where to Look: High-Impact Automation Opportunities in Healthcare
Administrative and Patient Access Workflows
The front end of the patient journey is the easiest place to start and often delivers measurable ROI within weeks.
Appointment reminders are a clear win. A 2022 US randomized study found that primary care no-show rates dropped from 9.1% with one text reminder to 8.4% with two, and mental health no-show rates fell from 20.1% to 17.9%. In high-volume practices, that reduction directly affects revenue and care continuity.
Insurance eligibility verification is a near-pure efficiency gain. Fully electronic eligibility checks could save the medical and dental industries $12.3 billion annually, and 96% of medical eligibility transactions were already electronic in 2023. The gap is in organizations still running manual spot-checks.
Prior authorization is where automation has the most concentrated impact. Only 35% of medical prior authorizations are fully electronic, yet automation could save 14 minutes per authorization - and physicians average 40 PAs per week.
Automating form population, submission, and status tracking removes one of the biggest sources of physician frustration without requiring clinical judgment from the system.
Revenue Cycle and Billing Workflows
The claims lifecycle is dense with automation opportunity, from charge capture through denial management. Key targets:
- Claim scrubbing and submission - automated validation catches coding errors and missing information before submission, targeting the industry benchmark of a 95%+ clean claim rate
- Eligibility-related denial prevention - registration errors caused 24% of 2023 denials; front-end automation closes that gap before claims are ever submitted
- ERA posting and A/R follow-up - automated payment reconciliation reduces manual matching work and provides real-time visibility into aging accounts
One caution: public data on automation-attributed first-pass rate improvements is limited. Use your organization's internal baseline denial rate and rework costs as the ROI anchor, not vendor-published benchmarks.
Clinical and Care Coordination Workflows
Two workflows here carry consequences beyond operational efficiency:
- Critical result notification - a 2023 ICU pilot found 61% of critical lab results acknowledged via push notification within 5 minutes, and 81% within 10 minutes. Automated escalation chains (EHR inbox → secure message → SMS alert) ensure closed-loop communication with a full audit trail.
- Care transitions and discharge coordination - nearly 2,300 hospitals were penalized by Medicare for high readmission rates in 2022, with HRRP reductions capped at 3% of base payments. Automated discharge workflows, referral management, and chronic care outreach reduce readmission risk by closing every handoff step that manual follow-up leaves open.
How to Prioritize: Building Your Automation Roadmap
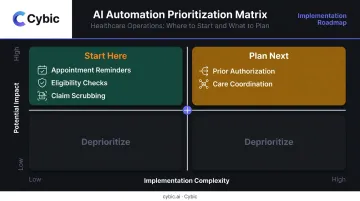
The Two-Axis Prioritization Model
Map your candidate workflows on two dimensions:
| Axis | What to measure |
|---|---|
| Potential impact | Staff hours saved, error rate reduction, revenue recovered, patient outcome improvement |
| Implementation feasibility | Integration complexity, data readiness, change management burden |
High-impact, low-complexity workflows go first. Administrative processes like appointment reminders, eligibility checks, and claim scrubbing typically land in this quadrant. Complex clinical automation - predictive risk scoring, autonomous care routing - comes after you've built the foundation and demonstrated ROI.
Map Before You Automate
Documenting the current-state workflow before selecting tools is not optional. A swimlane process map reveals:
- Cycle time at each step
- Handoff count and where delays accumulate
- Error injection points - where incorrect data enters the flow
Automating a poorly designed process just makes it fail faster. Organizations that skip this step often find themselves spending more fixing the automation than the original manual work cost.
Build Cross-Functional Input Into the Process
Bring clinical staff, billing teams, IT, and compliance officers into the prioritization conversation early. Front-line workers surface bottlenecks that don't show up in dashboards. Their input shapes better designs - and their buy-in drives adoption. Automation that bypasses the people closest to the work rarely sticks.
Key contributors to include:
- Clinical staff - identify workflow friction and patient-safety constraints
- Billing and coding teams - flag denial patterns and documentation gaps
- IT and integration leads - assess data readiness and system compatibility
- Compliance officers - define regulatory guardrails from the start
Pilot With Defined KPIs Before Enterprise Rollout
Start with a narrow workflow and define baseline metrics before you build: denial rate, time-to-result notification, staff hours on task. Measure against them after rollout, not after the fact.
Cybic's Drava platform is built for this phased model. It connects enterprise data, ML, AI reasoning, and intelligent agents under a governed framework - so teams can start with targeted workflows and expand without rebuilding from scratch.
Governance, Compliance, and AI Readiness in Healthcare Automation
HIPAA Is Architecture, Not a Feature
Every automated workflow touching PHI requires:
- Role-based access controls (RBAC) - not everyone who uses the system should see everything
- Encryption in transit and at rest - protecting data at every point in the pipeline
- Immutable audit trails - a record of every access, action, and decision
The critical mistake organizations make is treating these as features to configure post-deployment. Once an automation system is running, retrofitting access controls or audit logging into a working workflow is expensive and disruptive. Governance built into the architecture from day one avoids this entirely.
Cybic's approach embeds security controls, auditability, and regulatory alignment at the architecture level: compliance is a design requirement, not a checklist item. HHS OCR received 30,256 HIPAA complaints in 2024 and issued $8.76 million in monetary settlements. The enforcement environment is active.
AI Readiness: Data Quality Comes First
Before layering automation on top of existing systems, organizations need an honest assessment of their data:
- Is data consistently structured across EHR, billing, and departmental systems?
- Are there gaps or duplicates that would corrupt automated decision logic?
- Do legacy systems expose the APIs or data feeds that automation requires?
Only 43% of hospitals routinely engage in all four interoperability domains, per the 2024 ONC data brief. That fragmentation directly threatens automation projects that depend on clean, structured data flowing between systems. Cybic's data governance framework - covering landscape audits, gap analysis, and HIPAA-aligned policy - treats this as a prerequisite to deployment, not an afterthought.
Change Management Is as Important as the Technology
Staff adoption determines whether automation delivers its intended ROI. The framing matters: automation positioned as administrative burden relief - rather than a headcount threat - sees significantly better uptake.
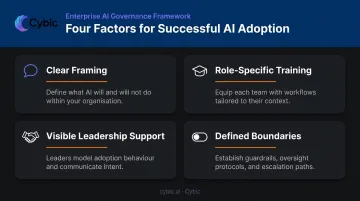
Four factors drive successful adoption:
- Clear framing: communicate what the system handles so staff understand its scope and limits
- Role-specific training: tailored to each team's interaction with the workflow
- Visible leadership support: signals organizational commitment and reduces resistance
- Defined boundaries: explicit about what the system decides versus what humans still own
That combination is what separates a workflow that sticks from one that gets worked around.
Frequently Asked Questions
How do you identify which healthcare workflows to automate first?
Prioritize tasks that are high-volume, rule-based, and error-prone - especially those with cross-system handoffs. Administrative workflows like eligibility verification, appointment reminders, and claim scrubbing offer faster wins and lower implementation risk than clinical processes, making them the right starting point for most organizations.
What are the most common workflows automated in healthcare?
Appointment scheduling and reminders, insurance eligibility verification, claims scrubbing and submission, prior authorization tracking, critical lab result notifications, and discharge coordination are the most frequently automated processes. These cover both the administrative and clinical coordination layers of a typical care delivery operation.
How does AI-powered automation differ from basic workflow automation in healthcare?
Basic automation handles predefined rule-based steps reliably and consistently. AI automation extends that capability by processing unstructured data like clinical notes, learning from historical patterns, and handling documentation variability that rules-based systems can't accommodate. Most organizations benefit from starting with rule-based automation before layering in AI capabilities.
What are the risks of automating healthcare workflows?
The main risks include:
- Automating a broken process amplifies existing errors rather than correcting them
- Inadequate HIPAA governance exposes PHI
- Poor system integration causes data loss at handoff points
- Staff resistance creates workarounds that defeat the automation entirely
All four are avoidable with proper process mapping, governance design, and change management.
How important is HIPAA compliance when selecting a healthcare automation platform?
It's non-negotiable. Any platform handling PHI must support role-based access controls, encrypted data handling in transit and at rest, and full audit logging. The vendor should also be willing to execute a Business Associate Agreement (BAA) - without one, the engagement creates direct regulatory exposure for your organization.