
Neither problem is hypothetical. Both signal the same underlying truth: HIPAA compliance isn't a box to check during onboarding. It's the daily operational framework that determines how your organization handles, shares, protects, and accounts for patient data across every system and vendor relationship.
This guide covers who must comply, what the four core rules require, how to build a compliant program, what violations look like in practice, and how AI deployments are reshaping the compliance surface area for healthcare organizations.
Key Takeaways
- HIPAA (1996) establishes federal standards protecting PHI across healthcare providers, insurers, clearinghouses, and their vendors.
- Four rules govern compliance: the Privacy, Security, Breach Notification, and Omnibus Rules.
- Compliance requires risk assessments, written policies, workforce training, Business Associate Agreements, and incident response plans.
- Civil penalties run $145–$2.1M+ per violation category; willful violations can result in criminal charges and imprisonment.
What Is HIPAA and Who Must Comply?
HIPAA - the Health Insurance Portability and Accountability Act of 1996 - started as a fix for two problems: health insurance portability between jobs and reducing healthcare fraud. Its privacy and security framework quickly became the dominant focus. Today, it defines the compliance infrastructure every healthcare organization operates within.
Covered Entities
Three categories of organizations are directly regulated:
- Healthcare providers that transmit health information electronically in covered transactions (claims submissions, eligibility queries, referral authorizations)
- Health plans - insurers, HMOs, Medicare, Medicaid programs
- Healthcare clearinghouses that process nonstandard health data into standard formats
Organization size does not determine compliance obligations. A solo physician practice submitting electronic claims carries the same legal exposure as a hospital system.
Business Associates
Any vendor or contractor that handles PHI on behalf of a covered entity is a business associate. This includes:
- EHR vendors and billing companies
- Cloud storage and hosting providers
- Legal counsel and auditors with PHI access
- IT service providers and managed service providers
Under the 2013 Omnibus Rule, business associates share direct compliance liability - not just contractual exposure through their covered entity clients. Subcontractors who handle PHI for business associates carry the same obligation.
What Counts as PHI
Protected Health Information is any individually identifiable health data in any format - written, oral, or electronic - tied to an individual's health condition, care, or payment.
HHS identifies 18 specific identifiers. Common examples include:
- Names, addresses, and phone numbers
- Social Security numbers and medical record numbers
- IP addresses and full-face photographs
- Dates beyond the year for individuals over 89
ePHI (electronic PHI) is the subset governed specifically by the Security Rule. Any digital system that stores, processes, or transmits patient data - from EHR platforms to cloud data pipelines - falls under its requirements.
The Four Core HIPAA Rules Explained
Privacy Rule
The Privacy Rule governs all permissible uses and disclosures of PHI. Key requirements:
- Treatment, payment, and healthcare operations are permitted without patient authorization
- Most other disclosures require written patient consent
- Minimum necessary standard applies - only share the PHI actually needed for the stated purpose
- Patients have the right to access their records (within 30 days, with one 30-day written extension), request amendments, and receive an accounting of disclosures
- Covered entities must provide a Notice of Privacy Practices (NPP) in plain language
Security Rule
The Security Rule applies specifically to ePHI and requires three categories of safeguards:
| Safeguard Category | Key Requirements |
|---|---|
| Administrative | Written policies, designated Security Officer, workforce training, risk analysis, access management |
| Physical | Facility access controls, workstation security, device and media controls |
| Technical | Access controls, audit controls, integrity mechanisms, encrypted transmission |

The Security Rule is "scalable" - controls must be reasonable and appropriate for the organization's size, complexity, and risk profile. Scalable does not mean optional. Smaller practices have proportionately adjusted obligations, not reduced ones.
Breach Notification Rule
Most breaches are discovered after the fact - which is why the Breach Notification Rule defines exactly what happens next. When a breach occurs, covered entities must:
- Notify affected individuals within 60 days of discovery
- For breaches affecting 500+ individuals in a jurisdiction: notify media outlets and report to HHS OCR immediately
- All 500+ breaches are posted publicly on HHS's breach portal - widely called the "Wall of Shame" - creating lasting reputational consequences
Omnibus Rule (2013)
Published January 25, 2013, the Omnibus Rule closed a critical gap: HIPAA's original framework placed obligations primarily on covered entities, leaving business associates largely outside direct liability. The rule changed that. Key updates include:
- Extended direct HIPAA liability to business associates and subcontractors
- Shifted the breach presumption - notification is now required unless a covered entity can document a low probability of compromise
- Extended PHI protections to 50 years post-death
- Strengthened patient rights around PHI use
Building a HIPAA-Compliant Program
Security Risk Assessment
A formal, written Security Risk Assessment (SRA) is the starting point for any compliance program. It must:
- Identify where ePHI is stored, transmitted, and accessed
- Evaluate threats and vulnerabilities across the environment
- Inform a prioritized remediation plan with documented decisions
The SRA must be reviewed at least annually and updated when significant operational changes occur - new systems, new vendors, new workflows. It's the first item auditors examine during an OCR investigation.
Policies, Procedures, and Workforce Training
Written policies can't be borrowed from generic templates and left unchanged. They must be customized to the organization and cover Privacy, Security, and Breach Notification requirements.
All workforce members - employees, contractors, volunteers, students - require HIPAA training at hire and annually thereafter, with documented attestation. Most real-world violations trace back to undertrained staff, not malicious actors - a pattern that documented, role-specific training directly addresses.
Designated Compliance Officers
Two roles are required by name:
- Privacy Officer - responsible for privacy policies, patient rights, and NPP compliance
- Security Officer - typically IT-background, responsible for technical safeguards, risk management, and Security Rule implementation
These are active, documented roles with defined responsibilities - not honorary titles assigned to whoever seems available.
Business Associate Management
Covered entities must:
- Maintain a complete inventory of all business associates
- Execute HIPAA-compliant Business Associate Agreements (BAAs) before sharing any PHI
- Review BAAs annually and update them when relationships or data flows change
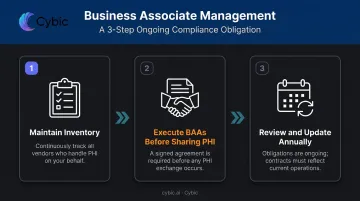
A covered entity can be held liable for a business associate's violations if it "knew or should have known" of a pattern of non-compliance. Vendor due diligence is an ongoing obligation, not a one-time contract signature.
Incident Response and Documentation
Every organization needs a documented process for identifying, investigating, and responding to potential breaches - including breach risk analysis, notification protocols, and remediation steps.
All compliance activities must be retained for a minimum of 6 years from creation or last effective date. Records that must be retained include:
- Audit logs and risk assessments
- Training records and attestations
- Executed BAAs and vendor due diligence files
- Breach investigations and incident reports
Documentation is the primary defense during an OCR audit.
For organizations deploying AI and data systems in clinical or operational workflows, compliance-aligned architecture is not optional. Platforms built for healthcare environments should incorporate role-based access controls (RBAC), encryption in transit and at rest, and full traceability of AI-driven actions - so that audit evidence is captured automatically, not assembled after the fact. Cybic builds these controls into system architecture from the start, rather than treating them as a post-deployment add-on.
Common HIPAA Violations, Penalties, and How to Avoid Them
Common Violation Categories
OCR enforcement data consistently identifies the same failure patterns:
- Impermissible use or disclosure of PHI - sharing records with the wrong party, discussing patient information in non-private settings
- Insufficient ePHI safeguards - unencrypted devices, weak access controls, internet-exposed servers
- Patients denied access to records - a top enforcement priority in recent enforcement cycles
- Failure to follow the minimum necessary standard
- Missing or inadequate Business Associate Agreements

Two OCR enforcement cases show the real cost:
- Lifespan Health System (2020, $1,040,000) - A stolen, unencrypted laptop exposed patient PHI. The absence of encryption policies and device inventory controls converted a theft incident into a HIPAA violation.
- iHealth Solutions (2023, $75,000) - A network server containing PHI of 267 individuals was left unsecured and accessible on the internet. Basic internet-exposure checks weren't in place.
The distinction matters: a stolen laptop is a breach. The absence of an encryption policy is what makes it a HIPAA violation.
These cases also reveal the penalty structure OCR uses to scale consequences - from good-faith oversights to willful neglect.
Civil and Criminal Penalties
Civil penalty tiers (2026 inflation-adjusted figures):
| Tier | Per-Violation Range | Annual Maximum |
|---|---|---|
| Did not know | $145 – $73,011 | $73,011 |
| Reasonable cause | $1,461 – $73,011 | $73,011 |
| Willful neglect, corrected | $14,602 – $73,011 | $73,011 |
| Willful neglect, not corrected | $73,011 – $2,190,294 | $2,190,294 |
Criminal penalties under 42 U.S.C. § 1320d-6:
- Knowing violations: up to $50,000 and 1 year imprisonment
- Violations under false pretenses: up to $100,000 and 5 years
- Violations for commercial gain or malicious harm: up to $250,000 and 10 years
HIPAA Compliance in the Age of AI and Digital Health
Healthcare AI adoption is accelerating fast. ONC data shows that hospitals' use of predictive AI integrated with EHRs rose from 66% in 2023 to 71% in 2024. Every new deployment - clinical decision support tools, predictive analytics platforms, AI-assisted documentation - expands the HIPAA surface area.
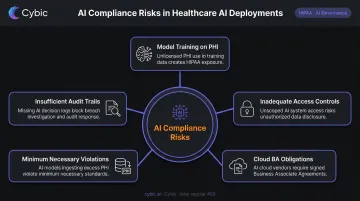
Where AI Creates New Compliance Exposure
Specific risks that AI introduces into healthcare environments:
- Model training on PHI without proper authorization or de-identification
- Inadequate access controls in multi-tenant cloud environments where ePHI flows across system components
- Insufficient audit trails for AI-generated clinical decisions - creating gaps in the documentation OCR would require
- Minimum necessary violations when large patient datasets are used for AI development without appropriate scoping
- Cloud service providers maintaining ePHI - even encrypted "no-view" services - qualify as business associates under HHS guidance and require BAAs
Each of these risks sits squarely within existing HIPAA enforcement territory. HHS has signaled increasing scrutiny of AI and health data uses, and no AI-specific exception exists. If PHI flows into a model, analytics tool, or AI platform, the full compliance framework applies: minimum necessary analysis, de-identification requirements, BAA obligations, and Security Rule safeguards.
Building Compliance Into AI Architecture From Day One
Retrofitting compliance onto an already-deployed AI system is expensive, disruptive, and incomplete. Organizations that embed governance controls at the architectural level avoid that problem entirely.
Cybic's healthcare AI engagements are structured around this principle. Every solution ships with:
- RBAC for role-scoped access to ePHI and system functions
- End-to-end encrypted data protection in transit and at rest
- Auditability and traceability of AI-driven actions at the level OCR requires
- A strict no-training policy - proprietary client data, including patient PHI, is never used to train models
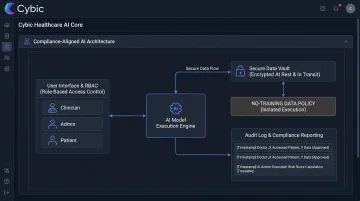
These controls are embedded in the architecture at build time, not configured after the fact.
For healthcare organizations evaluating AI vendors, the right questions are: Does your vendor require a BAA before any PHI-adjacent work begins? Can they produce audit logs granular enough for OCR review? Is data governance enforced by the system architecture, or dependent on manual process? And if something goes wrong, can your vendor demonstrate exactly what happened and when? The answers determine whether compliance is built in or bolted on.
Frequently Asked Questions
What is the key to HIPAA compliance in healthcare?
Consistent execution across four areas: ongoing risk assessments, documented policies and procedures, regular workforce training, and active monitoring of vendors and systems. Compliance is a continuous operational practice, not a one-time implementation, and requires documented evidence at every step.
What are HIPAA rules in healthcare?
Four primary rules govern HIPAA: the Privacy Rule (permissible PHI uses and patient rights), the Security Rule (ePHI safeguards), the Breach Notification Rule (notification timelines and requirements after a breach), and the Omnibus Rule (extended BA liability and updated definitions established in 2013).
Are autopsy reports covered by HIPAA?
Yes. HIPAA protects health information of deceased individuals for 50 years after death, so autopsy reports containing individually identifiable health information are generally covered. Coroners and medical examiners may access PHI under law enforcement and public interest exceptions, though disclosure must stay limited to the authorized purpose.
Who is required to comply with HIPAA?
Two groups: covered entities (healthcare providers submitting electronic transactions, health plans, and clearinghouses) and business associates (any vendor or contractor handling PHI on their behalf). Compliance obligations apply regardless of organization size.
What happens if you violate HIPAA?
Civil fines range from $145 to $2,190,294 per violation category annually under 2026 inflation-adjusted figures. Criminal penalties apply for willful misuse, including up to 10 years imprisonment for violations intended for commercial gain or malicious harm. Breaches affecting 500+ individuals are posted publicly on HHS's breach portal.
What is considered protected health information (PHI)?
PHI is any individually identifiable health information (written, oral, or electronic) relating to a person's health condition, care, or payment for care. The 18 identifiers specified under HHS de-identification guidance include name, Social Security number, medical record number, home address, dates of service, and IP addresses.


