
Introduction
HIPAA has governed patient health information in the U.S. since 1996, yet violations keep climbing. In 2024, OCR received 663 reports of breaches affecting 500 or more individuals - with over 242 million individuals affected, nearly double the previous year's total. That's not a blip. It reflects a compliance environment where organizations keep making the same structural mistakes.
Most violations don't trace back to nation-state hackers. They come from employee negligence, missing risk documentation, weak access controls, and vendors operating without proper agreements. These are fixable problems - when organizations treat compliance as an operational function rather than a documentation exercise.
This guide covers the most common violation types, what enforcement actually costs, how to spot compliance gaps before OCR does, and the practical controls that prevent violations before they occur.
Key Takeaways
- HIPAA violations happen when covered entities or business associates fail to protect, disclose, or manage PHI correctly
- Top violations: unauthorized PHI disclosure, employee snooping, missing risk analyses, weak ePHI access controls, and absent Business Associate Agreements
- Civil penalties range from $141 to $2,134,831 per violation category annually (2024 figures); criminal penalties reach $250,000 and 10 years imprisonment
- Effective prevention combines staff training, encryption, role-based access, regular risk assessments, and vendor oversight
- Sustained compliance requires governance built into daily workflows, not a once-a-year checklist review
The Most Common HIPAA Violations in Healthcare
HIPAA violations fall under three rules: the Privacy Rule, the Security Rule, and the Breach Notification Rule. OCR enforcement reveals a consistent pattern: organizations rarely violate just one provision. By the time investigators arrive, they typically find overlapping failures across multiple rules.
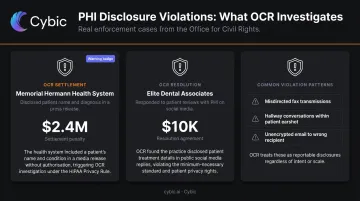
Unauthorized Disclosure of PHI
Impermissible PHI disclosure is consistently the most cited category in OCR enforcement - 660 complaints in 2024 alone. It covers a wide range of scenarios:
- Responding to patient reviews on social media with identifying details
- Faxing or emailing records to the wrong recipient
- Discussing patient cases in hallways, waiting rooms, or on phones where others can hear
- Including a patient's name or condition in press releases without authorization
Two cases illustrate how seriously OCR takes these disclosures. Memorial Hermann Health System paid $2.4 million after disclosing a patient's name in a press release. On the smaller end, Elite Dental Associates paid $10,000 for responding to patient reviews on social media with protected information. Size of organization doesn't determine whether OCR investigates. Pattern of conduct does.
Unauthorized Access to Patient Records (Snooping)
Accessing a patient's records without a legitimate clinical reason is a HIPAA violation regardless of whether you share the information. Curiosity, personal interest, or assisting a third party are not valid reasons.
Enforcement outcomes show the range of exposure:
- Montefiore Medical Center: $4.75 million settlement after an employee accessed 12,517 accounts and sold data to an identity theft ring
- UCLA Healthcare: A former employee received a federal prison sentence for illegally accessing patient records
- Northwestern Memorial Hospital: Dozens of employees terminated after inappropriately accessing Jussie Smollett's records
What makes snooping cases particularly damaging is that OCR doesn't need proof of harm - unauthorized access alone triggers liability.
Failure to Conduct Risk Analysis and Manage Security Risks
Under 45 CFR 164.308(a)(1)(ii)(A), every covered entity must conduct an accurate, organization-wide assessment of threats and vulnerabilities to ePHI. OCR's enforcement record shows that this requirement is violated constantly - and expensively:
| Organization | Settlement | Finding |
|---|---|---|
| Montefiore Medical Center | $4,750,000 | Failed to conduct risk analyses; no activity review mechanisms |
| Northeast Radiology, P.C. | $350,000 | Failed to conduct accurate and thorough risk analysis |
| BST & Co. CPAs, LLP | $175,000 | Failed to conduct risk analysis; ransomware investigation |
| Comprehensive Neurology, PC | $25,000 | Failed to conduct risk analysis after ransomware incident |
Completing a risk analysis isn't enough. Organizations that identify vulnerabilities and take no corrective action face the same enforcement exposure as those that skipped the analysis entirely.
Insufficient ePHI Access Controls and Encryption Gaps
Failing to limit ePHI access to authorized users, retaining terminated employees' system credentials, and leaving portable devices unencrypted are among the most penalized technical violations under the Security Rule.
Encryption is technically listed as an "addressable" specification under HIPAA - meaning organizations can document an equivalent alternative instead. In practice, skipping encryption without implementing and documenting that alternative creates enormous liability when devices go missing:
- University of Rochester Medical Center: $3 million settlement for failing to encrypt mobile devices
- Lifespan Health System: $1.04 million settlement after an unencrypted stolen laptop breach
- Concentra Health Services: $1.7 million for stolen unencrypted laptops
"Addressable" doesn't mean optional. It means document your rationale or encrypt.
Consequences of HIPAA Violations: What's Really at Stake
Civil Penalties
HHS adjusts HIPAA civil penalties annually for inflation. Under the 2024 figures (45 CFR 160.404), penalties break down across four tiers:
| Tier | Per-Violation Minimum | Per-Violation Maximum | Annual Cap |
|---|---|---|---|
| Unknown violation (reasonable diligence applied) | $141 | $71,162 | $2,134,831 |
| Reasonable cause, no willful neglect | $1,424 | $71,162 | $2,134,831 |
| Willful neglect, corrected within 30 days | $14,232 | $71,162 | $2,134,831 |
| Willful neglect, not corrected within 30 days | $71,162 | $2,134,831 | $2,134,831 |

OCR considers the harm caused, the number of individuals affected, and the organization's compliance history when setting penalty amounts. As of October 2024, OCR had collected $144.8 million across 152 resolved cases.
Criminal Penalties
The Department of Justice handles criminal HIPAA prosecution under 42 U.S.C. 1320d-6:
- Knowing violation: up to $50,000 and 1 year imprisonment
- Violation under false pretenses: up to $100,000 and 5 years
- Intent to sell or exploit PHI for personal gain: up to $250,000 and 10 years
Beyond the Dollar Amounts
Financial penalties are rarely the most disruptive outcome. Most significant OCR settlements also include:
- Corrective Action Plans (CAPs) that require rebuilding policies from scratch under direct OCR monitoring - Montefiore's ran two years
- Mandatory workforce retraining programs that consume staff time and budget
- Potential exclusion from Medicare and Medicaid programs
- Operational disruption as staff shift from patient care to compliance remediation
- Patient trust erosion that's difficult to quantify but compounds over time
Warning Signs Your Organization Has HIPAA Compliance Gaps
Compliance gaps don't usually announce themselves. They build quietly through outdated policies and overlooked daily practices - surfacing only when an audit or breach forces the issue.
OCR's 2016–2017 HIPAA Audit results make the scale of the problem clear: 94% of audited covered entities failed to implement appropriate risk management activities, and 89% couldn't document adequate compliance with individual right of access.
Outdated or Absent Policies and Risk Documentation
Watch for these red flags:
- No documented organization-wide risk analysis completed within the past year
- Business Associate Agreements not reviewed since before the 2013 Omnibus Rule - which required updated BAAs by September 23, 2014
- Privacy and Security policies that don't reflect current operations - for example, organizations that adopted telehealth platforms or new EHR systems without updating their documentation
Weak Access and Device Controls
Common technical warning signs include:
- Shared login credentials among staff (violates the unique user identification requirement at 45 CFR 164.312(a)(2)(i))
- Audit log monitoring that's inactive or never reviewed
- Former employees retaining system access after termination
- Unencrypted laptops or mobile devices used to access or store ePHI
Insufficient Training and Reporting Culture
Signs that staff accountability is thin:
- HIPAA training happens only at onboarding, with no annual refresher
- No anonymous channel for employees to report suspected violations
- Incidental disclosures - hallway conversations, visible monitor screens in waiting areas - treated as minor non-issues rather than compliance risks worth tracking
How to Prevent HIPAA Violations
Prevention isn't a single policy document. It's a layered system across technical controls, staff behavior, vendor relationships, and governance structures.
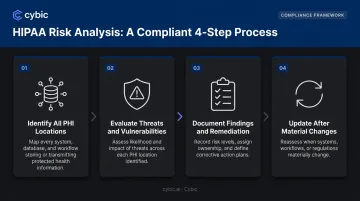
Conduct Regular, Documented Risk Analyses
A proper risk analysis under HIPAA requires more than filling out a template. It should:
- Identify all PHI locations : every system, device, and workflow where PHI is created, stored, or transmitted
- Evaluate threats and vulnerabilities - assess both likelihood and potential impact
- Document findings and remediation steps - the analysis is only valuable if it drives action
- Update after material changes : new EHR platforms, remote work expansion, mergers, and AI tool adoption each require a fresh analysis, not just an annual calendar reminder
NIST SP 800-66 Rev. 2 (finalized 2024) provides practical implementation guidance for the HIPAA Security Rule and is worth reviewing for any compliance team building or refreshing their risk management program.
Implement Technical Safeguards: Access Controls and Encryption
Role-based access controls (RBAC) are the foundation of ePHI security. Each staff member should only access the PHI their specific role requires. Access should be automatically reviewed when roles change and revoked promptly when employment ends.
Combined with RBAC, organizations should prioritize:
- Encryption of ePHI both at rest and in transit
- Unique user authentication (required under 45 CFR 164.312(a)(2)(i))
- Automatic workstation logoff after inactivity
- Regular audit log reviews to catch unusual access patterns early
For healthcare organizations deploying AI-powered clinical tools or data platforms, the architecture of those systems matters as much as the features. Cybic's enterprise AI solutions embed RBAC, encrypted data protection, and auditability directly into the system architecture - so compliance requirements are addressed at the design stage rather than retrofitted after deployment.
Execute and Maintain HIPAA-Compliant Business Associate Agreements
Any vendor, contractor, or technology provider that creates, receives, maintains, or transmits PHI on your behalf must have a signed BAA in place before any PHI is shared. The Center for Children's Digestive Health learned this the hard way - OCR found they had shared PHI with a records storage vendor since 2003 with no signed BAA, resulting in a $31,000 settlement.
Key BAA management practices:
- Review and update agreements after major regulatory changes
- Audit your vendor list periodically - shadow IT and new SaaS tools are common BAA gaps
- Holding a signed document is not sufficient; organizations remain responsible for monitoring BA compliance
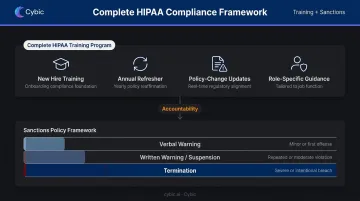
Train All Staff and Establish a Sanctions Policy
A complete training program includes:
- Initial training for all new hires, regardless of prior HIPAA experience
- Annual refresher training for all staff
- Targeted updates when policies change or new systems are introduced
- Role-specific guidance for staff with regular PHI access
Pair training with a written sanctions policy applied consistently from entry-level employees to physicians. Progressive consequences - verbal warning through termination depending on severity and intent - establish accountability. Without a sanctions policy, training is unenforceable.
Long-Term HIPAA Compliance Practices
HIPAA compliance isn't a project with a completion date. Regulations evolve, technology changes, and every new tool or workflow introduces potential exposure. Organizations that treat compliance as an ongoing governance function, rather than something they revisit under pressure, handle enforcement scrutiny far better.
Routine Monitoring, Audit Logs, and Breach Preparedness
Under 45 CFR 164.312(b), organizations are required to have mechanisms that record and examine activity in ePHI systems. Activating those mechanisms isn't enough - someone needs to actually review them.
Practical ongoing practices:
- Review audit logs regularly, with specific attention to access patterns following employee terminations
- Run periodic internal compliance audits, not just in response to complaints
- Maintain and test an incident response plan so the 60-day breach notification deadline can be met without scrambling
Documented breach readiness is an OCR compliance factor in its own right. Organizations that can demonstrate a tested response process fare better in investigations than those improvising after the fact.
Governance Embedded Into Technology and Workflows
AI tools are now standard in clinical and administrative operations. The compliance question is no longer whether a tool is technically compliant - it's whether compliance is built into how the tool works.
Platforms that embed audit trails, access controls, encrypted communication, and secure data handling at the architecture level reduce risk across the entire organization, not just within a single workflow. That's governance by design, not governance by inspection.
When evaluating clinical AI platforms, data pipelines, or analytics tools, look for systems where these capabilities are architectural defaults:
- Role-based access controls (RBAC) enforced at the system level
- Encryption applied in transit and at rest without manual configuration
- Audit trails that capture ePHI access automatically
- Auditability baked in, not bolted on post-deployment
Frequently Asked Questions
Frequently Asked Questions
What are the five most common HIPAA violations?
The five most frequently cited violations are:
- Unauthorized PHI disclosure without patient authorization
- Employee snooping on records without clinical justification
- Failure to perform an organization-wide risk analysis
- Insufficient ePHI access controls
- Missing or non-compliant Business Associate Agreements with PHI-handling vendors
What is an example of a HIPAA violation in healthcare?
A hospital employee accessing a celebrity's medical records out of curiosity - with no clinical reason - constitutes a violation even if nothing is shared externally. A practice that faxed records to the wrong number and missed the 60-day breach reporting window is another common example.
What are the financial penalties for HIPAA violations?
Under 2024 inflation-adjusted figures, civil penalties range from $141 per unknowing violation up to a $2,134,831 annual cap for uncorrected willful neglect. Criminal penalties for violations involving intent to sell or exploit PHI can reach $250,000 with up to 10 years imprisonment.
Can accidental HIPAA violations still result in penalties?
Yes. Unknowing violations carry civil penalties starting at $141 per incident - unintentional disclosure does not exempt an organization from liability. OCR considers intent when setting amounts, so unknowing violations draw lower minimums than willful neglect, but they remain penalizable.
Who enforces HIPAA compliance?
HHS' Office for Civil Rights (OCR) is the primary enforcement authority for the Privacy and Security Rules. The Department of Justice handles criminal prosecutions. State Attorneys General can also bring civil actions on behalf of residents.
What is a Business Associate Agreement and why is it required?
A BAA is a contract required under HIPAA whenever a vendor handles PHI on behalf of a covered entity. Sharing PHI with any third party without a current, signed BAA in place is itself a penalizable violation.


